
Purpose
This study investigated how multimodal sensory stimulation affected Glasgow Coma Scale (GCS) scores in stroke patients with decreased consciousness at Dr. Moewardi Hospital in Surakarta, Indonesia.
Methods
We employed a quasi-experimental approach with a pretest and posttest control group design. The control and intervention groups each contained 22 participants, all of whom were recruited via convenience sampling. The intervention group was given multimodal sensory stimulation (auditory, visual, olfactory, gustatory, and tactile) five times daily for a total of five days, with each session lasting 25 minutes. By contrast, the control group only received routine care from the hospital (i.e., no intervention). For statistical analysis, we used both the Wilcoxon test and Mann-Whitney test.
Results
We found a significant increase in posttest GCS scores for the intervention group (from 9.63 to 13.18, p=.001), but there was no significant increase for the control group (from 10.09 to 10.54, p=.085).
Conclusion
In this study, multimodal sensory stimulation effectively increased GCS scores in stroke patients with decreased consciousness. Nurses can use this intervention to improve sensory and GCS scores for such patients while in the intensive care unit.
This study investigated how multimodal sensory stimulation affected Glasgow Coma Scale (GCS) scores in stroke patients with decreased consciousness at Dr. Moewardi Hospital in Surakarta, Indonesia.
We employed a quasi-experimental approach with a pretest and posttest control group design. The control and intervention groups each contained 22 participants, all of whom were recruited via convenience sampling. The intervention group was given multimodal sensory stimulation (auditory, visual, olfactory, gustatory, and tactile) five times daily for a total of five days, with each session lasting 25 minutes. By contrast, the control group only received routine care from the hospital (i.e., no intervention). For statistical analysis, we used both the Wilcoxon test and Mann-Whitney test.
We found a significant increase in posttest GCS scores for the intervention group (from 9.63 to 13.18, p=.001), but there was no significant increase for the control group (from 10.09 to 10.54, p=.085).
In this study, multimodal sensory stimulation effectively increased GCS scores in stroke patients with decreased consciousness. Nurses can use this intervention to improve sensory and GCS scores for such patients while in the intensive care unit.
Stroke is both the second leading global cause of death after heart disease and the third leading cause of disability. Each year, there are approximately 16,000,000 new cases of stroke, with as many as 5,700,000 deaths. In the absence of population growth and adequate interventions, the annual number of stroke cases is estimated to increase to 23,000,000 by 2030 [1]. Data from the South East Asian Medical Information Center (SEAMIC) show that Indonesia ranks first in stroke mortality, followed by the Philippines, Singapore, Brunei, Malaysia, and Thailand [2]. According to diagnoses made by doctors, the Indonesian provinces with the highest and lowest percentages of stroke cases are East Kalimantan (14.7%) and Papua (4.1%) [3].
The dominant clinical symptoms of stroke include headache, vomiting, high blood pressure, and decreased consciousness [4]. Among these, decreased consciousness occurs when specific sensory stimuli in the forebrain are stopped or interrupted, thus affecting the Ascending Reticular Activating System (ARAS), which is one of the centers of consciousness [5, 6]. The loss of consciousness can be brief or slow depending on the severity of brain damage, with specific effects include respiratory problems, impaired physical mobility, impaired hydration, impaired swallowing, diminished communication skills, and impaired elimination [7]. In this context, shortening the loss of consciousness can improve outcomes and increase patient participation in rehabilitation [8]. Various nursing care efforts have been developed as non-pharmacological measures to increase patient awareness; for example, the nurse may adjust the patient’s head position to an elevation between 30° and 45°. Still, such approaches have not been maximized to quickly raise awareness [9]. While there is another form of therapy in sensory simulation, further developments are also needed to improve results [10].
The provision of appropriate and safe sensory stimulation can build synaptic connections to provide sufficient stimulation for ARAS. Stimuli with the right intensity and which are repeated correctly and accurately can increase the recovery rate of consciousness, thus facilitating the achievement of sensory function and reducing the duration of coma [11]. Stimulation content is based on the patient’s experience, with a family approach to fulfill the emotional element. In addition, stimulation is usually given through several sensory channels with different intensities, ranging from moderate to high [10]. Previous research has shown that multimodal stimulation involving visual, auditory, olfactory, tactile, and gustatory components can increase alertness/awareness in brain injury patients [12].
Multimodal sensory stimulation entails that smell, hearing, sight, taste, and touch are stimulated. As achieved through aromatherapy, olfactory stimulation can help release G-protein, thus increasing antibodies and improving blood circulation. Meanwhile, auditory approaches can stimulate nerve cells in the brain. For example, stimulation accomplished through music therapy can improve consciousness levels in severe head trauma patients. As for touch, stimulation therapy can enhance the blood flow system in returning blood to the cortical circulation system, thus effectively compensating for blockages that may cause stroke. Finally, stimulations of sight and taste can increase autonomic nervous system activity. By simultaneously targeting several senses that can stimulate ARAS, interventions can increase patient awareness and prevent ischemic brain cell damage [11, 12].
Several previous studies related to procedures for providing sensory stimulation have found that frequent intensities (five times per day) with short durations were better than long durations with low power (three times per day) [12]. Here, research has shown that providing sensory stimulation for 30 minutes at an intensity of two times per day can increase Glasgow Coma Scale (GCS) scores by 3 to 4 points in brain injury patients with decreased consciousness [8]. As sensory stimulation is a minimally invasive, harmless, inexpensive, and easy to apply, it has high potential as a method for increasing awareness. However, some studies suggest that the sensory stimulation method requires reform to achieve the desired goal [10]. This study expanded on previous research by involving family participation in providing patients with sensory stimulation. In this context, family members were the closest person to the patient and their primary sources of support. Here, we also hoped that such involvement would increase the overall role of the family in patient care. We chose to investigate stroke patients due to both the high number of cases and the lack of previous research on such a sample. Moreover, we ensured to recruit a relatively high number of participants in each study group.
A preliminary study involving the Intensive Care Unit (ICU) Rumah Sakit Umum Daerah (RSUD) Dr. Moewardi Surakarta over the last three months reported that there were 36 stroke patients with decreased consciousness. Their GCS scores varied from 9~12 (70%), 3~8 (20%), and 13~15 (10%). The preliminary study used observation sheets and standard operating procedures for GCS assessments. The results of interviews with nurses revealed limited collaboration in the context of drug administration and nasal cannula oxygen administration to increase patient awareness. Observations conducted on nurses and families revealed that they had provided unstructured sensory stimulation in the form of sensory sounds, namely by calling out the client’s name and simulating touch by holding the patient’s hand and face, but without any attention to the intensity, duration, form of stimulation, or assessment of its effects on the patient’s level of awareness. Based on the phenomenon of the problem and reviews related to previous studies regarding the sensory stimulation intervention, we developed an interest in determining how stimulation therapy would affect GCS scores in stroke patients with decreased consciousness.
This study used a quasi-experimental approach with a pretest and posttest control group design.
In this study, the sample included stroke patients with decreased consciousness. These participants were divided into intervention and control groups, with the control group only receiving standard hospital therapy (i.e., no intervention). The required sample number was calculated using the following formula:
Calculations were made using the results of previous studies, with details including SD=1.53; 1=7.14; 2=-5.65; Z1-α/2=1.96; Z1-β=1.28 [11]. Based on this formula, 22 participants were needed in each group. The requisite numbers were recruited via the consecutive sampling method, with predetermined inclusion and exclusion criteria. The inclusion criteria were: between middle adulthood (45~54 years) and older age (55~90 years), patients with stroke in less than 24 hours, GCS scores ranging from 9~13, normal blood glucose (100~200 mg/dL), and temperatures between 36.5~37.2℃. The exclusion criteria were: mortality before completion of the intervention (less than three days) and patients diagnosed with brain stem death.
All respondents signed informed consent forms as evidence of their willingness to participate in this study. After the researchers explained the nature of the research, one member from each family acted as the person in charge by signing the consent form. The family criteria were: nuclear family and lived in the same house as the patient. After obtaining ethical clearance from Universitas Diponegoro’s ethical commission, this study was conducted under the clearance number 471/EC/FK-RSDK/VII/2018.
Multimodal sensory stimulation simultaneously stimulates hearing, sight, touch, smell, and taste. In this study, GCS was used to measure the level of consciousness through both a pretest and posttest [12]. The pretest GCS value was the result of the GCS assessment prior to multimodal sensory stimulation, while the posttest GCS value was the result of the GCS assessment after receiving multimodal sensory stimulation on the last day of the intervention. The instrument reliability test was in the form of an operational procedure sheet using Cronbach’s α, with reliability established through a result of .85.
The interventional tools consisted of auditory, visual, tactile, olfactory, and taste stimulation devices. More specifically, visual stimulation was conducted by presenting family photos, while olfactory stimulation was accomplished by applying the patient’s favorite scent (perfume), and gustatory stimulation was accomplished using machines that applied lemon juice, various other flavoring essences, and cotton buds. In this study, multimodal sensory stimulation was conducted according to standard operating procedures with proven reliability. GCS scores were documented on the observation sheets.
This study was conducted at the ICU RSUD Dr. Moewardi in Surakarta, Indonesia from August to October of 2018. Data collection was first carried out for the intervention group, from August 1 to September 19, 2018. Data collection for the control group was carried out after the number of subjects in the intervention group had been met; that is, from September 20 to October 29, 2018. The data collection process was carried out by the researcher and three assistants, the latter of which were on-duty nurses with the ICU at Dr. Moewardi Surakarta and who met the researcher’s criteria; the researcher explains to the assistants about the research process to understand and have the same perception about the research process. The families of patients were involved in the provision of therapy. Prior to this, the researchers provided health education related to the vital role of family participation in providing multimodal sensory stimulation. As mentioned, provisions included auditory stimulation, visual stimulation, tactile stimulation, olfactory stimulation, and gustatory stimulation.
The pretest GCS scores of both groups were measured at the beginning. The control group was not exposed to any interventional therapy, but only received standard care from the hospital. The intervention group received the sensory stimulation multimodal treatment. Hearing stimulation was given by calling the patient’s name and sharing memories with the patient for five minutes at a distance of 10 cm from both ear canals. The stimulation was provided by the family calling the patient’s name three times, then describing family memories involving the patient until time ran out. Visual stimulation was given for five minutes by showing family photos to the patient at a distance of 10 cm from the eyes; if the patient’s eyes closed, then the nurse helped reopen them. Touch stimulation was given for five minutes, in which family members touched and gently rubbed the patient’s shoulder, then shook and gently rubbed the back of the patient’s hands. Olfactory stimulation was given for five minutes, with the researcher providing aromatic stimulation via the scent typically used by the patient at a distance of three cm from the nostril; specifically, the scent was the patient’s favorite perfume. Gustatory stimulation was given for five minutes, in which researchers applied lemon juice and various other essences/flavorings to a cotton bud that was touched onto the tip of the patient’s tongue.
Each stimulation lasted for a duration of five minutes so that each sensory stimulation session lasted for 30 minutes. Multimodal sensory stimulation was given to subjects in intervention group five times daily for five days and delivered five times/day, with at two-hour intervals. At the end of the intervention, all groups were measured using posttest GCS scores. The research sample received rewards in the form of digital sphygmomanometers, with the intention that families and patients would use the devices to monitor blood pressure.
Descriptive statistics were computed for all variables, including the minimum, maximum, means, Standard Deviations (SDs) for continuous variables, and frequencies and percentages for categorical variables. The normality analysis included the Shapiro-Wilk test, showing that the data were not normally distributed. As such, a bivariate analysis was conducted to assess the pretest and posttest data for each group using the Wilcoxon test. The differences between groups were then analyzed using the Mann-Whitney test.
As shown in Table 1, there were equal numbers of male and female stroke patients, with the most common type of stroke being hemorrhagic (59.1%). The majority of the intervention groups were men (72.7%), with the most common kind of stroke being non-hemorrhagic (59.1%). The test for homogeneity on gender and stroke type revealed p>.05, meaning that the sample was homogeneous. For study respondents, the average age was 56.90 years, with a serum glucose level of 111.25 g/dL. The test for homogeneity on age and blood sugar levels revealed p>.05, meaning that the sample was homogeneous.
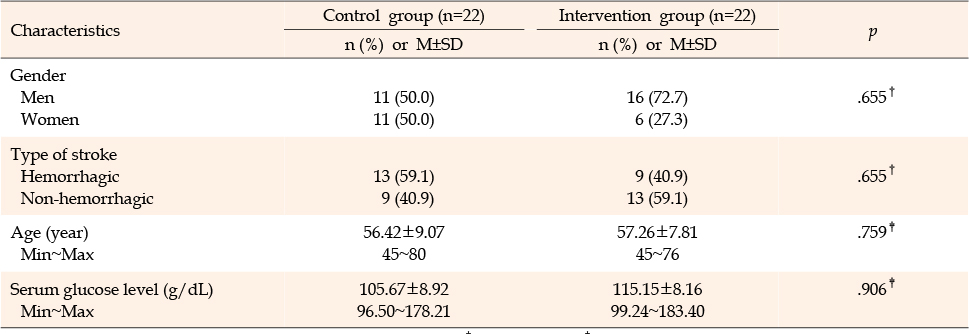
Table 1
The Homogeneity Test of Two Groups
As shown in Table 2, the intervention group showed a significant increase in GCS scores, moving from 9.63 to 13.18. However, the control group did not show a significant increase, only moving from 10.09 to 10.54. As also shown in Table 2, the control group did now show any significant differences in GCS scores between pretest and posttest (p=.085). The results of the bivariate analysis on the intervention group showed p=.001, meaning that the multimodal sensory stimulation intervention affected GCS scores in stroke patients, with an increase in the mean GCS score of 3.55 on the posttest. While a comparison of pretest scores between the control and intervention groups showed no difference (p=.319), a comparison of the posttest scores between the control and intervention groups did show a difference (p=.001). The results of the bivariate posttest-pretest difference between the control and intervention groups were p<.001, meaning there was a difference in GCS values between groups, in which multimodal sensory stimulation had an effect on the intervention group as compared to the control group. The difference between GCS scores in the intervention and the control group was 3.09.
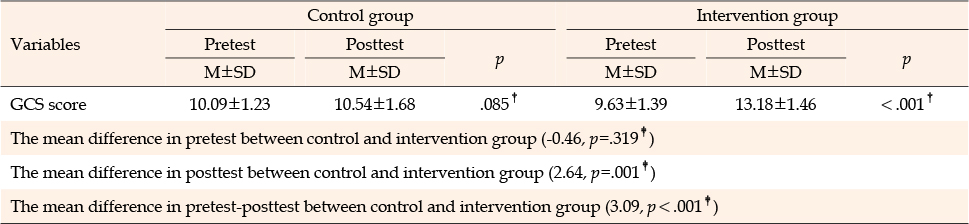
Table 2
Effects of a Multimodal Sensory Stimulation Intervention in GCS Score in Stroke Patients
This study investigated how stimulation therapy affected stroke patients. Based on the location of the brain disturbance, stroke patients may experience decreased consciousness. Previous studies have found that 13~48% of stroke patients experience delirium [9]. Decreased consciousness is one of the most common disorders among stroke patients, with studies showing that as many as 70% of patients may have GCS scores ≥9 [13, 14, 15]. Stroke patients may also experience intracranial hemorrhage, which has proven correlations with decreased consciousness [16]. Stroke patients with reduced consciousness require special treatment from nurses in addition to their regular care provisions. Megha et al. found a significant difference in GCS scores among head injury patients who were given sensory stimulation therapy when compared controls [12]. While previous studies have employed sensory and tactile stimulation in similar contexts [17], none have investigated multimodal sensory stimulation therapy in stroke patients with decreased consciousness
Sensory stimulation programs can promote brain plasticity and recovery in injured brains. It is associated with changes in cortical thickness, neuron size, and the number of connections. Appropriate and safe sensory stimulation can build synaptic connections to provide sufficient stimulus for the ARAS, thus increasing awareness [18, 19, 20]. Sensory stimulation has positive effects on brain metabolism, sympathetic activity, the release of norepinephrine in nerve terminals, and both awareness and arousal [21, 22]. This study employed auditory, visual, tactile, olfactory, and gustatory stimuli.
Previous studies have focused on unimodal stimulations, including many on auditory stimulation alone [4, 11, 23, 24, 25]. Other have investigated combinations such sensory and tactile stimulation [17] and auditory and tactile stimulation [22]. This study expanded on the literature by employing a multimodal stimulation intervention. In this regard, there is evidence that combined stimulation approaches are more effective than unimodal stimulations [26]. Moreover, regular and structured sensory stimulation programs can improve sensory function in stroke patients with impaired consciousness [27]. In multimodal sensory stimulation, the primary auditory cortex still responds to sound even with decreased consciousness [28].
While this study employed the same multimodal therapy provisions found in previous research [7, 12, 18, 27], there were some interventional differences. First, this study recruited a different sample from that used in Lumbantobing, with respondents having head injuries regardless of whether they showed decreased or normal consciousness. However, there were similar results in that intervention patients showed increased GCS scores after multimodal stimulation [7]. In Megha et al. [12], a physiotherapist examined three groups of brain injury patients, with a Western Neuro Sensory instrument used to measure consciousness. The results showed that the multimodal approach could stimulate consciousness levels in coma patients [12]. The difference with Moattari et al. [18] lies in the research sample, as those researchers examined patients with head injuries. In addition, some groups received interventions from nurses, with different evaluation tools used to assess results. In addition to GCS, the Rancho Los Amigos (RLA) and Western Neuro-Sensory Stimulation Profile (WNSSP) were used. The results were still similar in that multimodal stimulation did affect the level of consciousness in patients [18]. A similar study by Sargolzaei et al. [27] examined head injury patients, but did not implement gustatory stimulation. Sound stimulations were employed in the form of music and recordings, but not directly. Although the same type of stimulation was given, there were some differences in the tools and administration methods. Still, those results also showed increased consciousness in patients [27].
Unconscious patients require more help from nurses than other patients. Here, multimodal sensory stimulation therapy constitutes an easy and cost-effective approach that does not impose harmful effects. Families can also become involved to help increase awareness through this type of therapy. Zuo et al. [29] found that early sensory treatment provided by families was more effective than both routine care and implementation by nurses. However, nurses must educate families about the importance of sensory stimulation therapy and motivate them to implement it regularly. They can also provide teaching and assistance until families can perform the therapy independently. Unlike Megha et al. [12], who employed physiotherapy in one research group, this study involved the families of patients in the process of offering multimodal sensory therapy interventions.
Family contributions are important for synergizing the patient care process and achieving goals [30]. Multimodal sensory stimulation is a therapy in which the researcher collaborates with the patient’s family to provide auditory, visual, tactile, gustatory, and olfactory stimuli; here, both the intensity and frequency are adjusted to reflect each patient’s threshold for increased arousal and awareness. In this study, the researcher collaborated with the closest family member to the patient. Of the five senses that were given stimulation, the family played roles in providing auditory, tactile, and visual stimulations, while the researcher played roles in providing taste and smell stimulations. In previous research, a sensory stimulation program applied by family members was found to be more effective for increasing awareness in patients with head injuries than a program carried out by nurses for comatose patients, as determined based on GCS scores [31].
There is evidence that the voice of the patient’s mother or person closest to the patient has a more substantial effect on activating brain activity than an unknown voice [23]. This study used a similar approach to Tavangar et al. [25], who analyzed the voices of family members in a direct intervention. Still, other studies have used unfamiliar voices, such as Çevik et al. [32], who used the voices of male nurses, and Gorji et al. [11], who used voices recorded in the mp3 format. As an alternative approach, Sargolzaei et al. [27] used music and family sound recordings. Familiar sounds cause more neural responses than unfamiliar sounds. Nursing interventions that apply programmed sensory stimuli should be performed in the early stages of brain injury [22]. This study found that the use of programmatic family visits to provide mixed sensory (auditory, affective, and tactile) stimulation led increased awareness in the intervention group when compared to the control group. When used as part of a sensory stimulation program (significantly affective stimulation), this indicates that regular family visits may positively affect consciousness in patients.
The control group did not receive multimodal sensory stimulation over the three day study period, but showed slightly increased GCS scores. This may have been due to the administered drugs. This finding is in line with the results of previous research, in which the control group showed a GCS increase of 1.5 [12]. On the other hand, the intervention group showed a significant increase of 3.54 points in the GCS score. This finding supports previous reports that regular and structured sensory stimulation programs can improve sensory function in stroke patients with impaired consciousness [27]. If applied with the right intensity and repeated both correctly and accurately, such a program can increase the recovery rate of consciousness, facilitate the achievement of sensory function, and reduce the duration of coma [11]. Sensory stimulation performed immediately after the acute phase is recommended because it speeds recovery by preventing changes in plasticity and increasing patient awareness [4, 24].
This study had several limitations. First, the sounds made by life aids distracted auditory stimulation. The researchers overcame this by asking families to speak louder while still maintaining a soft tone. A second limitation was the differences in family educational backgrounds and ages. The researchers overcame this by repeatedly providing health education on multimodal stimulation until each family understood the information. This also meant that the frequency of education delivery differed between families, aiming to understand the intervention. In this regard, future studies should choose families with similar educational backgrounds and ages so that all education can be provided with the same frequency. Moreover, different family members may be available to care for patients on different days, meaning that the same individuals may not be able to consistently provide care over the intervention period. The researchers overcame this by setting the nuclear family as an inclusion criteria. As mentioned, the researchers also provided education to each participating family prior to intervention.
Based on this study’s findings, multimodal sensory stimulation plays an essential role in the recovery of stroke patients with impaired consciousness. As multimodal sensory stimulation is a collaborative process, nurses must also provide families with adequate health education. As a result in this context, nurses can improve sensory function and recovery in patients by providing an environment in which there is beneficial sensory stimulation. Continued research is needed to evaluate the effects of multimodal sensory stimulation over longer periods of up to two weeks, especially among stroke patients with decreased consciousness.
The results showed that multimodal sensory stimulation therapy effectively increased GCS scores in stroke patients when aided by nurses. That is, mean GCS scores increased in patients who received the therapy. The patient’s family is expected to play an active collaborative role in providing this therapy over the nursing care process. Nurses in special stroke units can incorporate multimodal sensory stimulation into existing interventions, especially for patients with decreased consciousness. Multimodal sensory stimulation therapy can be used both as an independent nursing intervention and in collaboration with the patient’s family.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design - FE, FS, and DY.
Data collection - FE and FS.
Data analysis and interpretation - FE, DY, KPD, and SM.
Drafting of the article - FS, RLN, KPD, and SM.
Critical revision of the article - FS.
This article is an extended study based on the first author's master's thesis from Diponegoro University.
This study received funding from an internal researcher.
The authors acknowledge all respondents, the Director of RSUD Dr. Moewardi, and the Head of Nursing HCU Anggrek II for their support in this research.
 E-SUBMISSION
E-SUBMISSION