
Purpose
This study investigated the factors associated with Adverse Event Following Immunization (AEFI) for Coronavirus Disease 2019 (COVID-19) in selected areas in Indonesia.
Methods
We used a cross-sectional approach with a correlational research design; a total of 2,730 samples were collected using accidental sampling. The instrument was an online questionnaire. The AEFI questionnaire was a modified version of the survey instrument of the Ministry of Health, Republic of Indonesia. χ2 and Fisher's exact tests were used for statistical analysis.
Results
The most common AEFI were pain at the injection site (81.2%), drowsiness (77.2%), hunger (77.0%), headache (70.3%), and weakness (58.4%). Bivariate testing revealed that gender, age, disease history, vaccine type, and anxiety had statistically significant relationships with the incidence of weakness, pain at the injection site, and headache (p<.050). Age and vaccine type were significantly related to the incidence of fever, swelling at the injection site, and hunger. Gender, vaccine type, and anxiety were found to have statistically significant relationships with the incidence of nausea. Vaccine type and anxiety were significantly related to vomiting.
Conclusion
The study found that gender, age, history of disease, vaccine type, and level of anxiety were associated with several adverse events following COVID-19 immunization. These findings provide data to nurses and other health workers to help them offer additional interventions to prevent or reduce adverse events in at-risk groups following COVID-19 vaccination.
This study investigated the factors associated with Adverse Event Following Immunization (AEFI) for Coronavirus Disease 2019 (COVID-19) in selected areas in Indonesia.
We used a cross-sectional approach with a correlational research design; a total of 2,730 samples were collected using accidental sampling. The instrument was an online questionnaire. The AEFI questionnaire was a modified version of the survey instrument of the Ministry of Health, Republic of Indonesia. χ2 and Fisher's exact tests were used for statistical analysis.
The most common AEFI were pain at the injection site (81.2%), drowsiness (77.2%), hunger (77.0%), headache (70.3%), and weakness (58.4%). Bivariate testing revealed that gender, age, disease history, vaccine type, and anxiety had statistically significant relationships with the incidence of weakness, pain at the injection site, and headache (p<.050). Age and vaccine type were significantly related to the incidence of fever, swelling at the injection site, and hunger. Gender, vaccine type, and anxiety were found to have statistically significant relationships with the incidence of nausea. Vaccine type and anxiety were significantly related to vomiting.
The study found that gender, age, history of disease, vaccine type, and level of anxiety were associated with several adverse events following COVID-19 immunization. These findings provide data to nurses and other health workers to help them offer additional interventions to prevent or reduce adverse events in at-risk groups following COVID-19 vaccination.
The Coronavirus Disease 2019 (COVID-19) outbreak is an ongoing global pandemic. The global incidence of COVID-19 as of December 29, 2021, was 281,808,270 cases, with 5,411,759 deaths. The number of active COVID-19 cases worldwide is 30,633,650 [1]. The United States of America accounts for the highest number of COVID-19 cases at more than 100 million, followed by Europe with more than 99 million. Southeast Asia ranks third, almost surpassing 50 million cases [2]. In the Republic of Indonesia, the number of cases had touched 4,263,433 as of January 3, 2022, with 144,102 deaths and 4,382 active cases [3].
The high incidence of cases, morbidity, mortality, and viral mutations continue to occur, underscoring the importance of control efforts so that COVID-19 can be suppressed. The World Health Organization states that education, isolation, prevention, transmission control, and treatment of infected people are essential for controlling infectious diseases such as COVID-19 [4]. Another main area of focus is COVID-19 vaccination [1]. Safe and effective vaccines have been developed and are being administered to people worldwide [5]. A total of 8,693,832,171 vaccine doses had been administered worldwide as of December 29, 2021 [2]. The target for vaccine recipients in Indonesia is 208,265,720, with first dose vaccine coverage reaching 80.0% and second dose coverage still at 55.0% [6].
Any vaccine can cause side effects, which are known as adverse events following immunization (AEFI); this also applies to COVID-19 vaccination. Research from Ontario presents AEFI data for COVID-19 vaccines from December 2020 to December 2021; the data provide a description of each adverse event according to the type of vaccine given. The most common AEFI are other severe or unusual events, allergic skin reactions, pain, redness, and swelling at the injection site, according to the data [7]. Jeon et al. [8] also researched AEFI for COVID-19 vaccination in the Republic of Korea using the Mobile Vaccine Adverse Events Reporting System (MVAERS) but did not analyze the associated factors. The results showed that malaise and tenderness and pain in the puncture area were the most common AEFI.
Tran et al.[9] researched the factors influencing AEFI in COVID-19 vaccination in Vietnam. The factors studied were age, gender, disease history, and vaccine type, but the results did not show a relationship between these variables and AEFI, which presented mainly as moderate fever, followed by fatigue, body ache, headache, pain at the injection site, and chills. A similar analysis was performed in Indonesia by Supangat et al.[10] who studied medical clerkship students. This study found similar AEFI such as fever, fatigue, weakness, sleepiness, drowsiness, body ache, headache, pain, and swelling at the injection site.
If AEFI in COVID-19 vaccination is not handled correctly, it can interfere with the subsequent vaccination process; people who experience AEFI during COVID-19 vaccination may have reduced motivation and be afraid to take the next immunization dose [11]. Previous studies have presented univariate data and variables on respondents' characteristics. There is hardly any research on anxiety over AEFI in COVID-19 vaccination. Research on factors related to AEFI in COVID-19 vaccination has never been carried out in Indonesia. Based on previous studies on AEFI in COVID-19 vaccination, the researchers carried out research on factors influencing AEFI in the first dose of COVID-19 vaccination in Indonesia.
This study aimed to determine the relationship that gender, age, disease history, type of vaccine, and anxiety had with adverse events after the first dose of COVID-19 vaccination in the Republic of Indonesia. Previous studies have separately examined the relationship between independent variables and the incidence of AEFI. This study aimed to present more complete data on the factors associated with AEFI. The variables of gender and age are irreversible factors that can be related to the incidence of AEFI. These variables were investigated to identify the groups at risk of developing AEFI so as to determine the appropriate treatment approach [9, 10]. History of illness is a factor that makes people hesitate to take the COVID-19 vaccine because they think it will make their disease worse [12, 13]. There are different types of vaccines given by the government; therefore, it is necessary to know their relationship with AEFI. Anxiety is also a factor that can be associated with AEFI [14]. Gender, age, disease history, vaccine type, and anxiety are the most discussed factors among all factors related to AEFI.
The research was a quantitative study that used a cross-sectional approach with a correlational research design.
The study included adult people who received the first dose of COVID-19 vaccination in Sleman District, Yogyakarta, Republic of Indonesia. The number of population is 311,530. The sample size was calculated using the Slovin formula [15]:
With details n=number of samples; N=number of the population; e=precision, the researcher used 5%. The required number of subjects was at least 400 based on the calculations. The total number of respondents who participated in this study was 2,730. The inclusion criteria specified that persons should be willing to be a respondent, be 26~55 years of age, and have completed at least elementary school. People who have been diagnosed with COVID-19, healthcare professionals, people who have a medical history of more than one disease, and people currently undergoing treatment for mental disorders were excluded. Accidental sampling was used to select a total of 2,730 participants.
The research was carried out after obtaining ethical clearance from the ethics committee of Universitas Respati Yogyakarta (No. 195.3/FIKES/PL/VIII/2021). Respondents first received an explanation of the purpose and process of the research and then signed an informed consent form as proof of their willingness to participate in the study. Respondents had the right to cancel their participation at any time and did not incur any penalties for doing so.
The instrument was a questionnaire consisting of three parts. The first part sought to determine the characteristics of the respondents (age, gender, and disease history) and the type of vaccine obtained. The questionnaire regarding the characteristics of the respondents was based on previous research [9, 10, 12, 13, 14]. For medical history, the respondents were asked to choose illnesses they suffered from a list. The choice of vaccine type depended on the vaccines provided by the government of the Republic of Indonesia, namely ChAdOx1 nCoV-19 (AstraZeneca’s COVID-19 vaccine) and CoronaVac (the Sinovac vaccine). The second part was a questionnaire on anxiety containing 20 statements. The anxiety questionnaire was adapted from D'Prinzessin [16]. The validity and reliability of the questionnaire were tested with 49 respondents. The validity test results showed that all statements had a rcount > rtable (rcount > .28). The reliability test results obtained a Cronbach’s α value of .92, indicating that the reliability of the instrument was excellent. The anxiety questionnaire contained four answer choices: "no" (score 0) if respondents do not feel anxious; "mild" (score 1) if they think about their anxiety but are not disturbed; "moderate" (score 2) if they think about it and it sometimes makes them uncomfortable; and "severe" (score 3) if they feel anxious and are very disturbed. Anxiety levels were divided into "no anxiety" (score 0), "mild anxiety" (score 1~20), "moderate anxiety" (score 21~35), and "severe anxiety" (score >35). Data collection was carried out before the COVID-19 vaccination.
The third part, the questionnaire on adverse events following COVID-19 immunization, was a modification of the instrument of the Ministry of Health of the Republic of Indonesia. The questionnaire consisted of 14 statements about the adverse events experienced after receipt of the first dose of the COVID-19 vaccine. The events were fever, cold, nausea, vomiting, weakness, drowsiness, swelling at the injection site, redness at the injection site, pain at the injection site, redness, itching and swelling in the eyes and mouth, itching in the body, headache, and hunger. Each statement was answered with a "Yes" or "No." Respondents could choose more than one AEFI depending on how they felt after receiving the first dose of COVID-19 vaccination. The questionnaire was tested for validity in 30 people, and the results showed rcount > rtable (rcount >.44). The reliability test results using Cronbach’s α yielded an α value of .85. The AEFI data were grouped into local AEFI and systemic AEFI. Local AEFI included swelling at the injection site, redness at the injection site, and pain at the injection site. Systemic AEFI included redness in the body, fever, cold, nausea, vomiting, weakness, drowsiness, itching and swelling in the eyes and mouth, itching in the body, headache, and hunger.
The study was conducted in Sleman District, Yogyakarta, Indonesia, from September to November 2021. The researchers contacted the Sleman District Health Office through the Sleman Regional Nurses Association Organization to request the COVID-19 vaccination schedule. Ten assistants helped the researchers in data collection. The assistants explained the entire research process to ensure a uniform perception. The researchers met potential respondents when they were scheduled to receive the first dose of vaccination, and explained the aims and objectives of the study to them while they were in the waiting room before vaccination. Those who were willing to participate in the study provided a phone number registered in the WhatsApp Messenger application. WhatsApp Messenger was developed by Meta Platforms, Inc., and originated in California, USA [17]. Respondents filled out a self-reported questionnaire about anxiety that was administered online via a Google Form with the link http://bit.ly/KecemasanPenerimaVaksinCovid-
Respondents also filled out a self-reported questionnaire about AEFI via a Google Form with the link http://bit.ly/KejadianPascaVaksinasiCovid_
Data were analyzed using the IBM SPSS 20.0 program. Descriptions of age, gender, disease history, type of vaccine, level of anxiety, and details of post-immunization co-occurrence were presented as frequencies and percentages. After the bivariate test, the dummy disease history variables became "Yes" or "None". Bivariate tests between the dependent and independent variables were performed using the χ2 test, while unqualified variables were analyzed using Fisher's exact test.
As shown in Table 1, the majority of respondents were women (67.8%) and in their early adulthood (57.2%). The majority of respondents did not have a history of comorbidities (55.0%), and the level of anxiety was mild (55.7%). Most respondents received the AstraZeneca vaccine (60.1%). The responses to the AEFI questionnaire showed that respondents experienced all AEFI with an incidence >70.0%, including pain at the injection site (81.2%), drowsiness (77.2%), hunger (77.0%), and headache (70.3%). Most respondents experienced fever (68.3%) and weakness (58.4%).
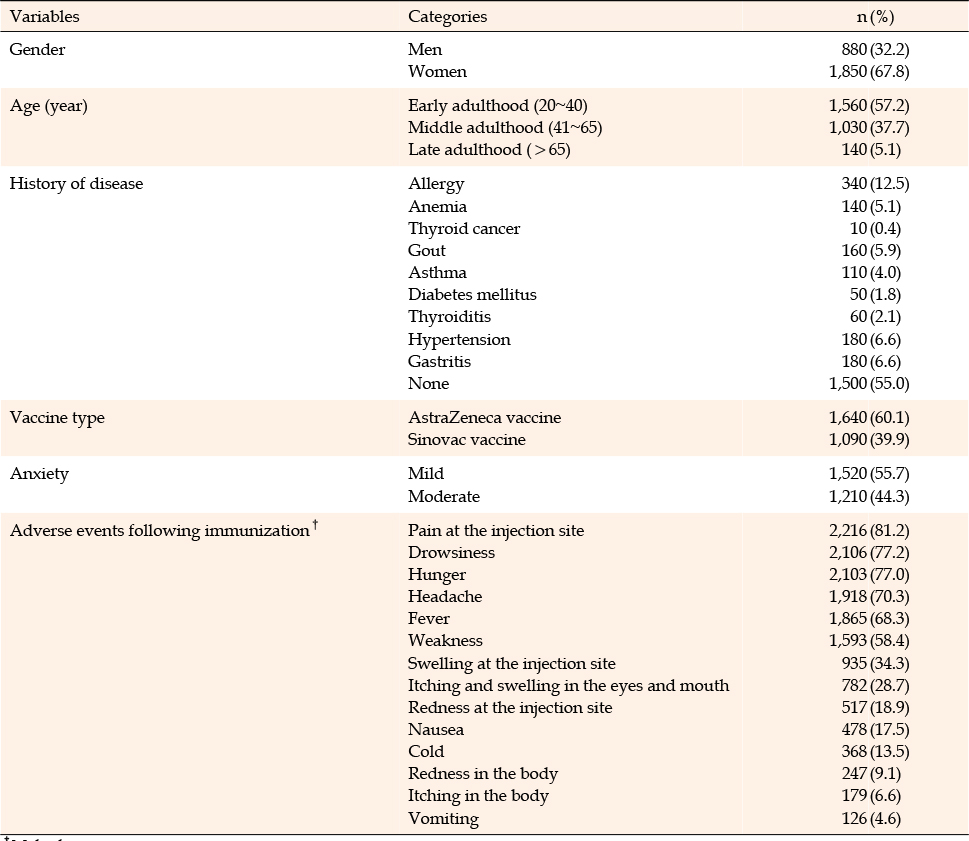
Table 1
Distribution of Characteristic Respondents (N=2,730)
In this study, AEFIs were categorized as local and systemic. Table 2 shows that all independent variables were associated with a local reaction in the form of pain at the injection site: gender (χ2=4.44, p=.035), age (χ2=38.77, p<.001), disease history (χ2=4.26, p=.017), vaccine type (χ2=32.23, p<.001), and anxiety (χ2=4.65, p=.032). The results showed that age (χ2=13.06, p<.001) and vaccine type (χ2=23.68, p<.001) had a relationship with a local reaction in the form of swelling at the injection site. None of the independent variables were associated with injection site redness or redness in the body (p>.050).
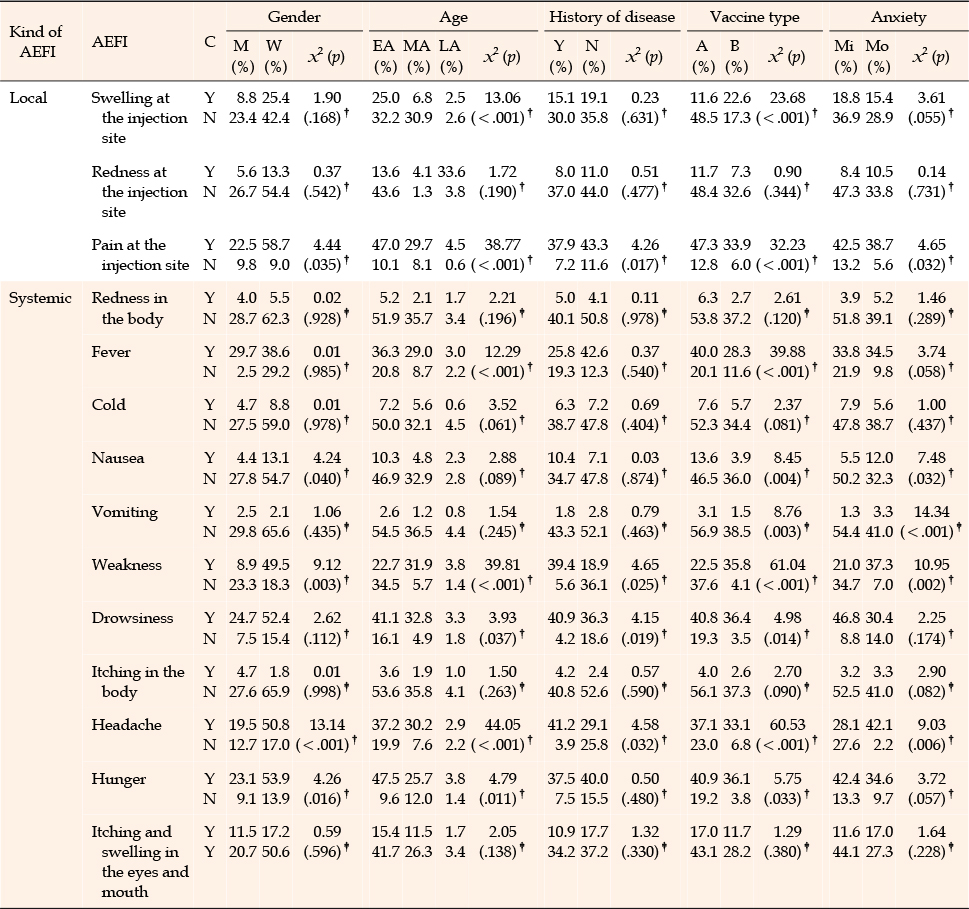
Table 2
Factors Associated with Adverse Events Following Immunization According to Characteristics of Participants After First Dose of COVID-19 Immunization (N=2,730)
Table 2 also shows the bivariate test results of the relationship of the independent variables with systematic AEFI. The results showed that all independent variables were associated with weakness: gender (χ2=9.12, p=.003), age (χ2=39.81, p<.001), disease history (χ2=4.65, p=.025), vaccine type (χ2=61.04, p<.001), and anxiety (χ2=10.95, p=.002). All independent variables were also associated with headache: gender (χ2=13.14, p<.001), age (χ2=44.05, p<.001), disease history (χ2=4.58, p=.032), vaccine type (χ2=60.53, p<.001), and anxiety (χ2=9.03, p=.006). Factors associated with the incidence of nausea were gender (χ2= 4.24, p=.040), vaccine type (χ2=8.45, p=.004), and anxiety (χ2=7.48, p=.032). Vaccine type (χ2=8.76, p=.003) and anxiety (χ2=14.34, p<.001) were also associated with vomiting. Factors related to hunger were gender (χ2=4.26, p=.016), age (χ2=4.79, p=.011), and vaccine type (χ25.75, p=.033). Factors related to drowsiness were age (χ2=3.93, p=.037), disease history (χ2=4.15, p=.019), and vaccine type (χ2=4.98, p=.014). The results showed that age (χ2=12.29, p<.001) and vaccine type (χ2=39.88, p<.001) had a relationship with the incidence of fever.
This study revealed the participants' condition when they received the vaccine and the effects after the first dose of COVID-19 vaccination. Data on AEFI in COVID-19 vaccinations have been presented in several scientific publications [7, 18] and are regularly featured on the government websites of countries such as the UK [19] and Canada [20]. This study revealed the participants' condition when they received the vaccine and the effects after the first dose of COVID-19 vaccination. All respondents experienced some sort of reaction in their bodies after vaccination; this result differs from the finding in a study by Tran et al.[9] in which 3.9% of respondents reported no post-vaccination effect. The most common AEFI in this study was pain at the injection site, followed by hunger, drowsiness, and headache. These results echo previous findings that pain at the injection site was the most commonly reported effect by vaccine recipients [21, 22, 23].
The study results differ from Ontario data, wherein other severe or unusual events were the most common AEFI, while pain at the injection site ranked third [7]. Supangat et al. [10] also conducted a study in the Republic of Indonesia and reported different results, with weakness being the most common effect experienced by respondents after vaccination. In the current study, incidence of weakness ranked sixth. Sebedi et al. [12] found that tenderness at the injection site was the most commonly reported AEFI. In this study, tenderness at the injection site was minimal, with none of the variables associated with this event. This study directly presents data on AEFI as perceived by the respondents.
Supangat et al. [10] found no correlation between AEFI symptoms and gender, with both men and women having the same chance of developing AEFI symptoms. This finding is different from the present study’s results: gender is related to AEFI such as nausea, weakness, pain at the injection site, and headache. The results are similar to those of previous studies, which found that women are more likely than men to experience AEFI [12, 13, 14]. Vaccine recipients aged 45~59 years were 50% less likely to develop AEFI than those aged less than 30 years [12]. Being young and female were risk factors for grade 3 to grade 4 local and systemic adverse reactions [14], as corroborated by a study by Klugar et al. [24]. These findings suggest that the incidence of each AEFI is higher at a younger age than at an older age. This differs from the findings of Lee et al. [14], who added nutritional status and other factors to the list of independent variables.
A history of illness is related to AEFI after COVID-19 vaccination. Patients with a history of allergies, hypertension, and neurological disorders exhibited anaphylactic reactions more often than those without such a history [25]. Lee et al. [14] added that people with diabetes mellitus are 2.36 times more at risk of developing AEFI than non-diabetics; they provided a data overview without relating it to AEFI. This study divided the categories into "yes" and "no" answers, so it was not possible to determine what type of disease history is associated with AEFI.
The Indonesian government provides two types of vaccines: Sinovac and AstraZeneca. Past studies have generally discussed only the side effects of the AstraZeneca vaccine [14, 26]. Riad et al. [27], on the other hand, examined only the side effects of the Sinovac vaccine. The results of this study support Ramasamy et al.’s [28] finding that the AstraZeneca vaccine appears to be better tolerated in older adults than in younger adults. The study results showed that vaccine type had a relationship with the incidence of AEFI; participants who got the AstraZeneca vaccine experienced more AEFI than those who got the Sinovac vaccine. Another difference is the sample used; previous research used health workers as respondents [24, 26, 27, 29].
In addition to personal characteristics, this study included respondents' anxiety. All study respondents were anxious before receiving the COVID-19 vaccination, with the symptoms ranging from mild to moderate. Prospective vaccine recipients are anxious because they think that vaccines and AEFI are dangerous and threaten their lives. These results are in line with those of Hause et al.[30], wherein COVID-19 vaccination participants in the United States complained of mild to severe anxiety with symptoms of fainting. This study shows that higher levels of anxiety lead to more AEFI events.
Statistically, the level of anxiety is associated with several AEFI, including nausea, vomiting, weakness, pain at the injection site, and headache. This finding supports that of Lee et al. [14], in which a significant percentage of respondents who experienced anxiety also experienced AEFI. Chen et al. [25] found that a history of anxiety or depression was associated with a higher risk of severe neurological AEFI. The results showed that the majority of respondents experienced mild anxiety. Anxiety is a condition involving physical, emotional, cognitive, and behavioral responses that arise in anticipation of situations considered dangerous. Mild anxiety is a reasonable daily level of anxiety because it can widen a person's field of perception, thereby helping individuals anticipate potential threats and take steps to overcome them [31].
The results of this study provide essential data for nurses about the possible side effects of COVID-19 vaccination in patients. Nurses can use this data to provide interventions to prevent or treat AEFI. Nurses generally provide health education about COVID-19 vaccination before the administration of the vaccine. Health education aims to increase knowledge and readiness regarding vaccination in the community. It also reduces people’s anxiety toward COVID-19 vaccination and equips them to be physically and mentally prepared before vaccination.
Nurses also teach patients how to handle AEFI when they actually occur. Good knowledge enables the community to recognize and treat AEFI early to prevent any negative impact. The study results also provide data about at-risk groups: women, older people, and those with a history of disease. Nurses need to pay special attention to these groups during pre-vaccine education, at the time of vaccination, and during post-vaccination monitoring. If AEFI after the first dose of the COVID-19 vaccine can be handled adequately, motivation to participate in the next vaccine drive is expected to increase. Taylor et al. [32] found that distrust of vaccine benefits and fear of vaccine effects were associated with resistance to COVID-19 vaccination.
This research was conducted through a survey using an online form. Subjects entered data on demographic characteristics and anxiety levels with the aid of researchers or assistants, so they could be controlled. However, data entry about AEFI was carried out without supervision from the researchers or assistants, so respondents could not immediately get clarification on anything they did not understand. However, an explanation was provided to respondents through a conversation via WhatsApp Messenger. In addition, the questionnaires were released using social media, so the study population was biased toward people who used social media, had Internet access, and were willing to participate. Researchers also did not continue processing multivariate data to determine the factors most related to the incidence of AEFI.
Furthermore, the researchers also limited the number and simplified the questions, raising the possibility of missing detailed information; this was done to obtain a large number of respondents. This study only showed the presence or absence of AEFI without exploring their severity. The education and knowledge factors of respondents were also not investigated, so the influence of respondents' knowledge about the introduction and treatment of AEFI could not be controlled. However, despite the limitations of this data collection method, this study applied a simple, economical, and contact-free approach and, importantly, could produce significant results in a short period.
The results showed that the most common adverse events following COVID-19 immunization were pain at the injection site, drowsiness, hunger, headache, and weakness. The events that appeared the least were redness, itching in the body, and vomiting. Nurses play a role in improving health by educating the public about adverse events following COVID-19 immunization and how to handle them. Education aims to minimize the effects without reducing people's motivation to take the next vaccination dose. Gender, age, history of disease, vaccine type, and level of anxiety were not associated with the incidence of redness at the injection site, redness in the body, itching and swelling in the eyes and mouth, and itching in the body. However, gender, age, history of disease, vaccine type, and level of anxiety were associated with several other adverse events following COVID-19 immunization. These findings provide data to nurses and other health workers about at-risk groups to help them offer additional interventions to prevent or reduce adverse events in these groups following COVID-19 vaccination.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design - FS and SDI.
Data collection - FS, SDI, MM, ATAE and PA.
Data analysis and interpretation - FS, MM, SR, and PA.
Drafting of the article - FS, SDI, MM, and SR.
Critical revision of the article - FS.
This study was funded by The Center for Research and Community Service, Universitas Respati Yogyakarta with a number of contract 021/Int/PPPM/V/2021.
The authors acknowledge all respondents, Sleman Sub-District and District Head who have given research permission.
 E-SUBMISSION
E-SUBMISSION