
Purpose
This study aimed to develop and examine the effects of a mobile application-based self-management program for Chemotherapy-Induced Peripheral Neuropathy (CIPN) in colorectal cancer patients.
Methods
This study used a nonequivalent control group and a pretest-posttest design. Eighty-three patients with colorectal cancer undergoing neurotoxic chemotherapy were included in the study (experimental group, n=41; control group, n=42).
The self-management program for CIPN consisted of an eight-week program (for individual training and telephonic coaching). CIPN 20, a CIPN assessment tool, and European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-C30 scale were used to assess CIPN, disturbance of activities of daily living, and quality of life, respectively. The study was conducted from December 7, 2018, to August 20, 2019. For data analysis, descriptive statistics, a test of homogeneity in the pretest, independent t-tests, and repeated-measures analysis of variance were used.
Results
In the experimental group, significant improvements were found in CIPN (F=5.88, p=.018) and disturbance of activities of daily living (F=8.26, p=.005) compared to those in the control group. There was no significant difference in the interaction between the groups and time in terms of quality of life.
Conclusion
Our results indicate that the mobile application-based self-management program used in this study is effective and could be used as a nursing intervention for cancer patients with CIPN.
This study aimed to develop and examine the effects of a mobile application-based self-management program for Chemotherapy-Induced Peripheral Neuropathy (CIPN) in colorectal cancer patients.
This study used a nonequivalent control group and a pretest-posttest design. Eighty-three patients with colorectal cancer undergoing neurotoxic chemotherapy were included in the study (experimental group, n=41; control group, n=42). The self-management program for CIPN consisted of an eight-week program (for individual training and telephonic coaching). CIPN 20, a CIPN assessment tool, and European Organization for Research and Treatment of Cancer Quality of Life Questionnaire-C30 scale were used to assess CIPN, disturbance of activities of daily living, and quality of life, respectively. The study was conducted from December 7, 2018, to August 20, 2019. For data analysis, descriptive statistics, a test of homogeneity in the pretest, independent t-tests, and repeated-measures analysis of variance were used.
In the experimental group, significant improvements were found in CIPN (F=5.88, p=.018) and disturbance of activities of daily living (F=8.26, p=.005) compared to those in the control group. There was no significant difference in the interaction between the groups and time in terms of quality of life.
Our results indicate that the mobile application-based self-management program used in this study is effective and could be used as a nursing intervention for cancer patients with CIPN.
Chemotherapy-Induced Peripheral Neuropathy (CIPN) is a common and severe adverse effect of chemotherapy [1, 2], which may develop weeks to months after exposure to chemotherapeutic agents, resulting in disturbances in daily activities and reduced quality of life [3]. Oxaliplatin, a cytotoxic platinum compound, is a chemotherapeutic agent used to treat colorectal cancer [4]. Approximately 48% of patients who receive oxaliplatin-based chemotherapy develop neuropathy symptoms during treatment, which may resolve after the treatment’s cessation. However, 20~50% of these patients experience chronic symptoms [5]. CIPN symptoms and levels are affected by various factors, including the type of anticancer drug, cumulative dose, nutritional status, treatment duration, underlying medical conditions (e.g., diabetes and alcoholic neuropathy) [6], and muscle mass [7]. Major symptoms of CIPN usually include sensory neuropathies (numbness and tingling of the hands or feet, or both, burning pain, and paresthesia) and motor neuropathies (muscle weakness and muscle cramps) [6]. An increasing number of colorectal cancer survivors suffer from negative and disabling consequences of CIPN, which affect their quality of life [2, 8].
To date, effective treatment options to prevent or decrease CIPN have not been reported, and symptoms of peripheral neuropathy have been resolved by discontinuing or reducing the doses of anticancer drugs [9, 10]. Accordingly, patients with cancer often choose to self-manage their CIPN symptoms without physician supervision [9, 11]. In this context, non-pharmacological interventions are being utilized to relieve the symptoms of CIPN, including acupuncture, massage, exercise, psychosocial mediation, and health supplements, as provided in the guidelines for integrated cancer treatment [9]. Most intervention studies have reported the effectiveness of health supplements containing vitamin E and Alpha-lipoic acid, which are antioxidants and traditional herbal extracts, respectively. However, no consistent results show that vitamin E has preventive effects on peripheral neuropathy [9]. In a recent meta-analysis [10], acupuncture and massage were reported to significantly relieve symptoms and pain related to CIPN. However, only four studies were included in the meta-analysis, suggesting the need for further verification. Exercise can attenuate motor deficits and improve inter-and intramuscular coordination, contributing to improved stability and gait [12]. Balanced exercise has been suggested as an effective intervention to relieve symptoms related to peripheral neuropathy in a meta-analysis study of people with diabetes and peripheral neuropathy [9, 12]. However, there are no consistent results regarding the effectiveness of exercise in cancer patients with CIPN. Therefore, whether such lifestyle factors could also play a role in the development and consequences of CIPN in patients with colorectal cancer needs to be investigated.
Mobile technologies, including smartphone applications, have emerged as new tools for delivering health-related services in the field of cancer [13]. Approximately half of all cancer-related applications are targeted toward breast cancer patients and are designed to provide disease and treatment information and manage the disease [13]. Mobile applications provide a great deal of flexibility in terms of time and location and offer learner-centered interventions through audio, video, and text material [13]. However, applications for managing CIPN symptoms in colorectal cancer are still in the early stages of development.
This study aimed to develop and estimate the effectiveness of a mobile application-based self-management program for peripheral neuropathy, a non-pharmacological intervention, in colorectal cancer patients undergoing neurotoxic chemotherapy. We hypothesized that eight weeks of a self-management program would improve CIPN symptoms. Our secondary research questions were related to the self-management program's effects on the disturbance in Activities of Daily Living (ADL) and quality of life measures.
This study used a single-blinded nonequivalent control pretest-posttest design.
There were 83 participants (experimental group, n=41; control group, n=42) included in this study. Patients with colorectal cancer were invited to participate in the study from a cancer center in Korea. Recruitment of participants started in December 2018, and the follow-up was completed in August 2019. The inclusion criteria were as follows: 1) age≥20 years; 2) receiving oxaliplatin-containing combination chemotherapy; 3) ability to walk without an assistive device; and 4) presence of CIPN symptoms (obtained from the patient charts). The exclusion criteria were assessed by chart review or patient self-report and included: 1) diabetes, 2) arthritis, and 3) neurological disorders including stroke and dementia. The experimental and control groups were conveniently selected, and the control group was selected from patients with similar general and disease characteristics, such as age, sex, and performance status, as the experimental group. The sample size needed for repeated-measures Analysis of Variance (ANOVA) was calculated using the G*Power program 3 [14]. A total sample size of 54 participants (27 in each group) was required for a significance level (α) of .05, power of .95, medium effect size (f2) of 0.25, and correlation among repeated-measures of .05, two groups, and two measures. We used an effect size of 0.25 based on a prior study [15], which reported a medium effect size of exercise on CIPN in patients with cancer. Considering the dropout rate, 50 participants were required for each group. Of the 50 patients invited, 41 were included in the experimental group. One participant did not meet the inclusion criteria, two answered insincerely, and six did not continue the intervention. A total of 42 patients were included in the control group; one patient did not meet the inclusion criteria, one refused to complete the follow-up assessment, three could not be reached, and three responded unfaithfully.
This study was approved by the Institutional Review Board of the Cancer Center in Korea (IRB N0: KIRAMS 2018-09-004-001). Patients received information on the eligibility criteria, purpose, and procedures of the study. Potentially eligible participants were provided with written informed consent forms, assuring the confidentiality of all information. Furthermore, participants could voluntarily withdraw without any adverse consequences. All the participants were provided with a small amount of compensation. After the post-test data were collected, a mobile application-based self-management program was provided to the control group.
We used the Korean version of the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ)-CIPN 20 developed by the EOTRTC-Quality of Life Group [16]. It consists of 20 items: nine sensory, eight motor, and three autonomic items. The questions were rated on a four-point Likert scale. The scale scores were linearly converted to a 0~100 scale, with higher scores indicating a greater symptom burden [17]. A previous study reported its initial development. The coefficients for the sensory, motor, and autonomic scales were .88, .88, and .78, respectively [18]. Cronbach’s α was.91 in this study, and the coefficients for the sensory, motor, and autonomic scales were .84, .86, and .43, respectively. We obtained permission from EORTC.org to use the tool.
The Korean version of the Chemotherapy-Induced Peripheral Neuropathy Assessment Tool (CIPNAT) was used [19, 20]. We used 14 disturbances in ADL from CIPNAT. The questions were rated on an eleven-point scale ranging from 0 to 10. The total score ranges from 0 to 140. Higher scores indicate greater disturbance in ADL. In a previous study reporting its initial development for use with cancer patients, Cronbach’s α was .90 [20]. The instrument's reliability was indicated by Cronbach’s α of .92 when standardized in Korean, and Cronbach’s α was .93 in this study. We obtained permission from the author to use CIPNAT.
We used the Korean version of the EORTC QLQ-C30 developed by the EOTRTC-Quality of Life Group [21]. It consists of 30 items: two global health status, 15 functional, and 13 symptom items. The global health items were rated on a seven-point Likert scale, and the functional and symptom items were rated on a four-point Likert scale. All scale scores were linearly converted to a 0-100 scale, with higher scores on global health status and functional scales indicating a better quality of life. Lower scores on the symptom scales also indicated a better quality of life [21]. In a previous study reporting its Korean version, Cronbach’s α coefficients were 0.81~0.92 [22]. In this study, the Cronbach’s αs for the global health status, symptoms, and function scales were .91, .91, and .85, respectively. We obtained permission from EORTC.org to use the tool.
The program was based on systematic reviews of nonpharmacological interventions for peripheral neuropathy in cancer patients [10], phenomenological studies of peripheral neuropathy experienced by patients with cancer [11], and interviews with experts. Additionally, the scope and content of the learning material contained in the app and booklet were determined by reviewing the literature and patient education booklets [9, 12, 23, 24, 25, 26].
The program consisted of education via an application, training (sensory stimulation training and exercise), and individual telephonic coaching. The mobile application structure consisted of four screens on the main screen: education, today's exercise, exercise records, and setup, with the training screen appearing first when the user logs into the app (Figure 1). Five experts evaluated the content validity of the self-management program: two clinical physical therapists, one oncology nurse specialist, one professor of oncology nursing, and one professor of kinetic therapy, on a four-point scale for each subject. The content for exercise methods was supplemented based on experts' feedback, and the program was finalized with a Content Validity Index (CVI) of over .80.
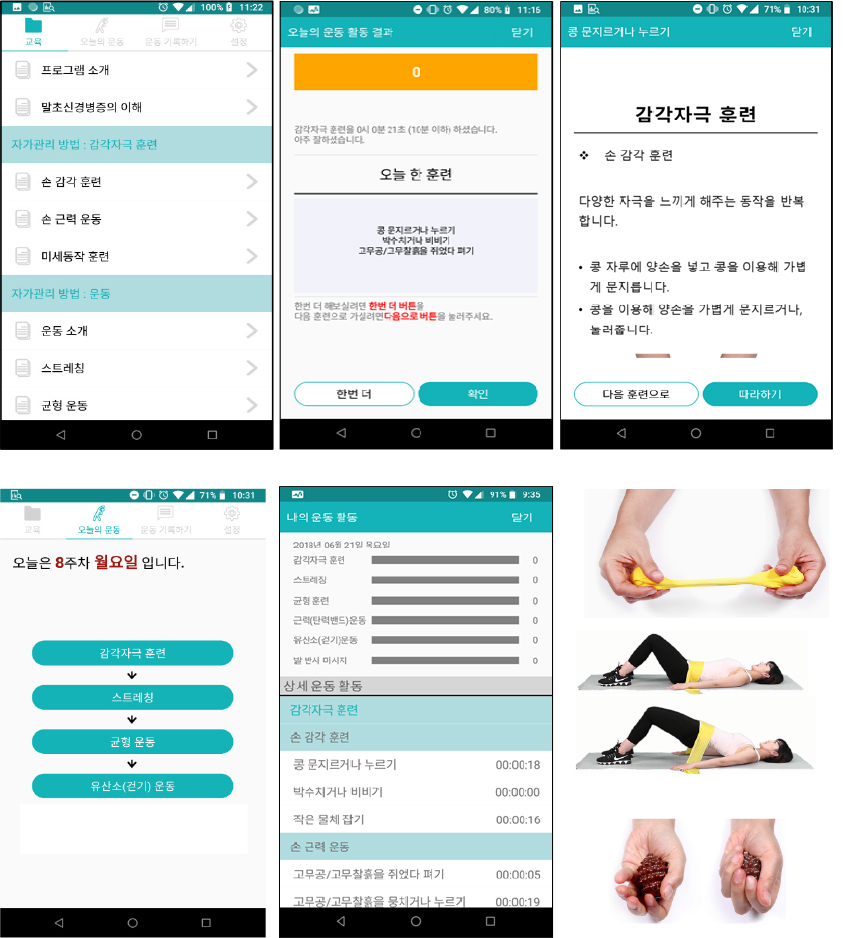
Figure 1
Mobile application: main pages.
The mobile application-based self-management program for peripheral neuropathy was delivered over eight weeks, three times a week, with each session lasting 10~30 minutes. The eight-week intervention was based on a meta-analysis study in which non-pharmacological interventions for alleviating CIPN symptoms were performed for an average of 8.6 weeks [10]. In the first session of the program, two researchers provided instructions via applications and booklets (Table 1). Program manuals were provided so that participants could use them by themselves. Session one covered the participants' assessment of peripheral neuropathy, utilization of the program, and peripheral neuropathy description. Instructional training for using the app was provided while conducting a questionnaire during the first week of the program. CIPN education dealt with topics such as the causes of peripheral neuropathy, symptoms, effects on daily life, and self-management methods. The session consisted of 30 minutes of application training and supplementary explanations, and a question-and-answer session was conducted via telephonic coaching. Session two specifically covered sensory stimulation training and exercise methods as self-strategies to relieve symptoms of peripheral neuropathy. Sensory stimulation training was designed to repeat motions such as placing both hands in a bean bag, rubbing hands using the beans, rubbing the palm or the back of the hands, and stretching and bending the fingers using therapeutic putty or a rubber ball [23, 24]. Education on exercise consisted of balancing, strength (elastic band), and aerobic (walking) exercises. Strength exercises and walking were performed thrice a week. Weeks 3~7 were individual action stages, where the participants were instructed to perform the content learned in sessions one and two at home. During this stage, two telephonic coaching sessions were conducted to support the participants’ symptoms, training progress, and provide feedback (Table 1). Adherence to physical activity was monitored on the manager page of the mobile app every two weeks at the start of self-training. Instruction training was conducted in a separate room or the participants’ ward, with a single participant or small groups of two to three participants.
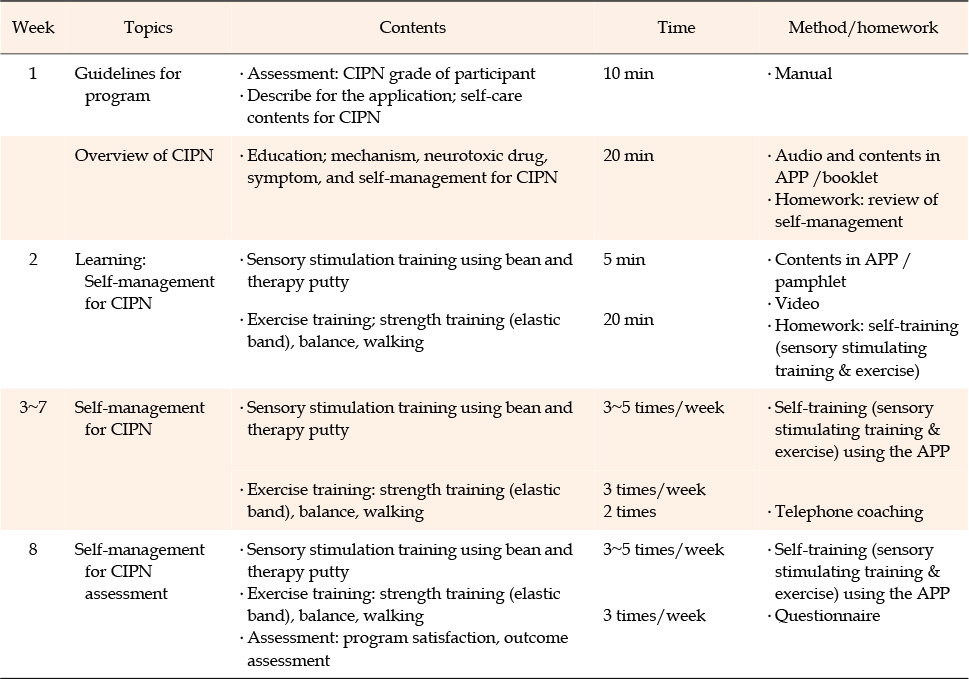
Table 1
Mobile Application Based Self-management Program for Chemotherapy-induced Peripheral Neuropathy
A booklet-based self-management program for peripheral neuropathy was applied to the control group. Two researchers provided instructions through booklets. The session lasted 10~20 minutes and covered the participants' assessment of peripheral neuropathy, its description, and self-management methods. Questionnaires were administered after data from the experimental group were collected.
Measurements were performed at baseline and after eight weeks in the Cancer Center clinic. Data from the pretest were collected from patients who visited the Cancer Center, met the selection criteria, and signed an informed consent form, agreeing to participate in the study. A questionnaire survey was conducted to measure peripheral neuropathy symptoms, disturbances in ADL, and health-related quality of life. The posttest was conducted by a researcher who was unaware of the group assignments.
Statistical Package for the Social Sciences version 23.0 (IBM Corp., Armonk, NY, USA) was used for all analyses. The participants' general and clinical characteristics were calculated using the frequency, percentage, mean, and standard deviation. Participant characteristics and between-group homogeneity of the dependent variables were analyzed using the χ2 test and unpaired t-test. The Shapiro-Wilk test, skewness, and kurtosis were used to verify the normality of the study variables. CIPN symptoms, disturbances in ADL, and health-related quality of life in the pretest-posttest or between groups were analyzed using a repeated-measures ANOVA.
A total of 83 patients participated in the study. Men accounted for 63.8% of the participants, and the mean age was 58.64 years (standard deviation=8.64). A majority of the participants (83.1%) were married, 54.2% had a high school education, 30.1% had graduated from middle school or less, and 59.1% did not have a job. Regarding monthly income, 48.2% earned less than KRW 2 million. Of the 83 participants, 61.4% had no metastases. Moreover, 66.3% of the participants had grade 1 Eastern Cooperative Oncology Group performance and ambulatory status, and the ability to perform light or sedentary work, and 53.0% had a chronic disease. The average dose of oxaliplatin was 1,281.79 mg (experimental group: 1,382.39 mg; control group: 1,181.19 mg). There were no statistically significant differences between the two groups in terms of participant characteristics (Table 2). In the homogeneity test of variables, no significant differences were found in CIPN (t=1.00, p=.316), disturbance of ADL (t=0.45, p=.651), or quality of life: functional (t=-0.34, p=.739), symptom (t=0.31, p=.761), and global health status (t=0.43, p=.663) between the two groups.

Table 2
Homogeneity Test of General & Clinical Characteristics between Experimental and Control Group (N=83)
There was a significant difference in the interaction between groups and time (F=5.88, p=.018). After the intervention, CIPN levels were lower in the experimental group than in the control group (Table 3). Among the sub-items, significant reductions in sensory symptoms were found (F=6.64, p=.012). No significant effects were observed for motor (F=1.33, p=.252) and autonomic (F=3.13, p=.080) CIPN symptoms in the experimental group. There was a statistically significant difference in CIPN symptoms in the experimental group before and after the intervention (t=3.53, p=.001). However, there was no significant difference in CIPN symptoms of the control group over time (t=-0.69, p=.489). The mean score for CIPN severity was 23.19 in the experimental group and 19.75 in the control group at baseline. The CIPN domain showed that most CIPN was sensory symptoms (experimental group: 28.31; control group: 24.36), followed by autonomic (experimental group: 26.96; control group: 22.62), and motor (experimental group: 15.79, control group: 13.36) symptoms at baseline.
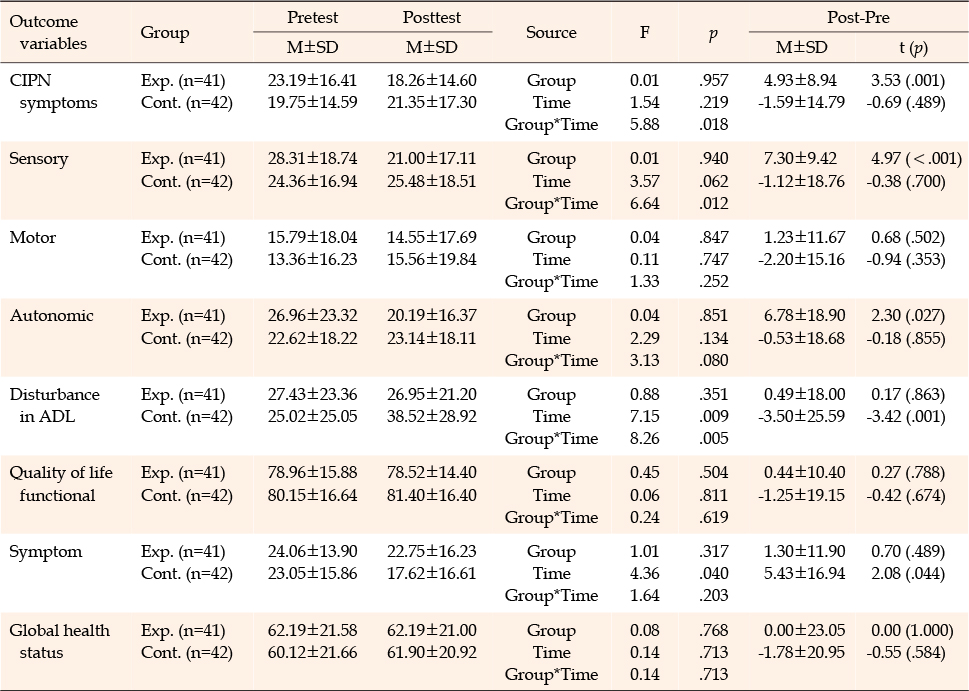
Table 3
Effects of a Mobile application based Self-management Program for Chemotherapy-induced Peripheral Neuropathy (N=83)
There was a significant difference in the interaction between groups and time (F=8.26, p=.005). ADL disturbance by CIPN in the experimental group using a mobile application-based self-management program was significantly lower than that in the control group (Table 3). There was no significant difference in disturbance in ADL of the experimental group before and after the intervention (t= 0.17, p=.863), but there was a significant increase in disturbance in ADL of the control group over time (t=-3.42, p=.001).
There were no significant differences in the interaction between time and group in the sub-items of quality of life: functional area (F=0.24, p=.619), symptom area (F=1.64, p=.203), and global health status (F=0.14, p=.713) (Table 3). The self-management program for CIPN had no significant effect on improving the quality of life.
This study aimed to develop and estimate the effectiveness of a mobile application-based self-management program for peripheral neuropathy in colorectal cancer patients undergoing neurotoxic chemotherapy. We observed significant reductions in the experimental group's sensory symptoms compared to the control group after eight weeks of the self-management program. These results are consistent with previous studies [10] that showed a medium effect size, indicating the significance of non-pharmacological interventions in relieving CIPN symptoms. In this study, a non-pharmacological self-management program consisted of CIPN education, sensory stimulation training, and exercise. We speculate that CIPN education helped enhance cancer patients' self-care behaviors by strengthening their self-efficacy through a comprehensive understanding of CIPN [26], thereby relieving the disorder’s symptoms. Moreover, sensory stimulation training helps relieve symptoms by stimulating the fingertips to promote sensory recovery of the hand [23, 24]. Participants were instructed to perform strength (elastic band) and aerobic exercises (walking) three times a week to promote recovery of the damaged peripheral nerve by enhancing blood supply [15]. Individual telephonic coaching feedback provided during our intervention may have particularly improved the process of self-management for CIPN control. The non-pharmacological self-management program used in this study could be a meaningful nursing intervention because it relieved symptoms in the sensory domain of patients with cancer. The major symptoms of CIPN are sensory disorders accompanied by numbness, tingling, hyperesthesia in the hands or feet, and burning pain [6, 11, 27]. Considering that these sensory nerve symptoms can affect motor skills, relief of symptoms in the sensory nerves may be preemptive for maintaining and managing motor skills [25]. While noticeable improvements were observed in the sensory symptoms of CIPN, no significant effects were found in its motor (muscle weakness and cramps) and autonomic nervous domain. Such results can be related to the participants' poor exercise performance, despite the two telephonic coaching based on the analysis of application monitoring. This could be because of the deterioration of their physical health, individual exercise at home, and the least number of symptoms in the motor domain compared to symptoms in the sensory nerves or the autonomic nervous system [11, 28]. These results are consistent with the findings of a previous meta-analysis, which reported that the effect of exercise on the balance and strength of patients with peripheral neuropathy was not statistically significant [10]. However, further verification is needed because only two studies on exercise were included in the meta-analysis, and five studies included in the systematic review suggested that exercise was effective in relieving CIPN symptoms [10]. Future studies could include the following possible actions for improving outcomes for colorectal cancer patients during chemotherapy treatment: higher intensity of physical activity, such as supervised exercise including individualized programs; inclusion of more telephonic coaching; and longer durations (>30 min) of physical activity. Approximately 1 h and 30 min of physical activity are needed to achieve an equivalent of 10,000 steps per day, which is a moderate level of physical activity [29].
Peripheral neuropathy impedes walking and coordination, increasing the risk of falls [30]. Chronic peripheral neuropathy continues even a year after chemotherapy completion [1, 2, 31], which requires monitoring and nursing interventions through exercise.
In this study, the experimental group did not show a significant decrease in ADL disturbances associated with peripheral neuropathy eight weeks after the program compared to before the program; however, the control group showed more severe ADL disturbances associated with peripheral neuropathy eight weeks after the program (average of 38.52) than during chemotherapy (average of 25.02). These results support previous findings that a higher number of chemotherapy cycles results in a higher cumulative dose of neurotoxic anticancer drugs, which increases the difficulty level in daily activities [32]. The toxic symptoms of peripheral neuropathy because of an increase in the number of chemotherapy sessions eventually disrupt daily activities. These ADL disturbances were relieved by non-pharmacological intervention in this study, showing its significance for CIPN in cancer patients undergoing chemotherapy.
In this study, the self-management program for peripheral neuropathy had no significant effect on cancer patients' health-related quality of life. This result is consistent with the findings of a previous meta-analysis, which showed that the effects of six non-pharmacological interventions on quality of life were not statistically significant [10]. However, the self-management program for peripheral neuropathy in this study was developed as an exercise and sensory stimulation training program that focuses on peripheral neuropathy. Although the quality of life of cancer patients was measured in functional and symptom areas (fatigue, nausea and vomiting, pain, shortness of breath, insomnia, loss of appetite, constipation, diarrhea, and financial problems) using an assessment tool for health-related quality of life, these areas did not include CIPN symptoms. In this study, participants’ scores for health-related quality of life were higher than those of patients with colorectal cancer studied by Kim et al [33]. Since CIPN symptoms were identified based on the participants' subjective reports in this study, it is necessary to measure and compare the degree of peripheral neuropathy with objective indicators in the future. Regarding the CIPN program, participants were provided with education on peripheral neuropathy during hospitalization and were instructed to perform sensory stimulation training for pain and exercise through self-training after discharge. After discharge, self-training was encouraged through telephonic coaching, but we did not control for the participants’ usual care and general physical activities.
This study was limited in terms of the participants’ self-training levels after discharge. Moreover, there are limitations to generalizing the program's effects since these were measured only immediately after the end of the program. Additionally, there are limitations in generalizing the study results owing to the convenient samples and low reliability (Cronbach’s α: .43) of the autonomic subscales of the EORTC QLQ-CIPN 20 questionnaire. Autonomic scale is consisted of 3 different items such as orthostatic hypotension, blurred vision & erection dysfunction with low internal consistency (.22~.24).
Replication studies on CIPN management programs using non-pharmacological interventions are required because only a few domestic studies have been conducted on this subject to date.
This study's findings suggest that a mobile application-based self-management program is safe and effective for decreasing patients' CIPN symptoms. Participants were instructed to perform sensory stimulation training and exercise through audio and video content, and individual telephonic coaching. CIPN symptoms were relieved, and disturbances in daily activities associated with CIPN were reduced. Therefore, active utilization of this self-management program for CIPN in the counseling and education of cancer patients undergoing chemotherapy is recommended as an independent nursing intervention. In the future, long-term longitudinal and replication studies are needed to determine the period during which self-management programs are effective. In particular, this program is expected to provide a new strategy for nurses in counseling and educating patients with cancer undergoing chemotherapy on self-management.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - OP-J.
Data collection - LJR.
Analysis and interpretation of the data - OP-J and LJR.
Drafting and critical revision of the manuscript - OP-J.
This research was supported by the National Research Foundation of Korea (NRF) funded by the Korea government (MSIT) (No. NRF-2017RIA2B1002950).
 E-SUBMISSION
E-SUBMISSION