
Purpose
Health behavior is important for the treatment of tuberculosis patients. This study aims to clarify the concept of health behavior in tuberculosis patients.
Methods
We used Rodger's evolutionary concept analysis method. A literature search was performed using the NDSL, NAL, RISS, PubMed, ProQuest, CINAHL, Web of Science and Cochrane Library published in Korean and English language from January 2015 to April 2021. After applying inclusion and exclusion criteria, a total of 69 articles were selected for final analysis.
Results
The analysis showed that five attributes determine health behavior concepts: willpower, the choice for every moment, counterbalance, overcoming, and multi-level multi-causal processes.
Conclusion
This study shows that health behavior in tuberculosis patients has evolved into a patient-centered approach in an evolutionary context. The results of this study will contribute to the development of intervention access and management programs for health care providers, including nurses.
Health behavior is important for the treatment of tuberculosis patients. This study aims to clarify the concept of health behavior in tuberculosis patients.
We used Rodger's evolutionary concept analysis method. A literature search was performed using the NDSL, NAL, RISS, PubMed, ProQuest, CINAHL, Web of Science and Cochrane Library published in Korean and English language from January 2015 to April 2021. After applying inclusion and exclusion criteria, a total of 69 articles were selected for final analysis.
The analysis showed that five attributes determine health behavior concepts: willpower, the choice for every moment, counterbalance, overcoming, and multi-level multi-causal processes.
This study shows that health behavior in tuberculosis patients has evolved into a patient-centered approach in an evolutionary context. The results of this study will contribute to the development of intervention access and management programs for health care providers, including nurses.
결핵은 한국과 전 세계의 주요 공중보건 문제이다. 세계보건기구(World Health Organization, WHO)에 의하면 2019년 전 세계적으로 약 1,000만 명의 결핵 환자가 발생했고 142만 명이 결핵으로 사망했다[1]. 한국의 결핵 신 환자 수는 2011년 최고치(10만 명당 39,557명) 이후 매년 7.3%씩 감소하고 있다[2]. 그러나 2019년 국내 전수 감시 대상 감염병 중 두 번째로 많은 신고 환자 수와 가장 많은 사망자 수, 그리고 경제협력개발기구(Organization for Economic Cooperation and Development, OECD) 36개 회원국 중 결핵 발생률 1위, 사망률 2위를 기록하며 결핵은 여전히 높은 발생을 보인다[1, 2].
2015년 “The End TB (tuberculosis) Strategy”를 발표한 WHO는 결핵 퇴치를 위해 통합된 환자 중심의 관리와 예방을 핵심으로 정부, 보건, 지역사회의 다양한 분야에서 적극적인 지지가 필요하다고 강조했다[3]. 현재 우리나라 국가결핵관리는 민간·공공협력 결핵관리사업을 통해 법 개정, 예방 홍보, 검진과 치료비 지원 등 다양한 전략을 추진하고 있다[4]. 또 협력의료기관의 결핵관리 전담간호사와 보건소의 결핵관리 담당자는 결핵 환자의 치료를 완료할 수 있도록 개별 결핵 환자 상담과 관리 활동을 수행하고 있다[2, 4]. 그러나 이는 국가결핵관리시스템 보고 위주로 환자의 의학적 상태 파악, 질환과 치료에 대한 정보 제공, 검사 결과, 복약 확인, 접촉자 확인과 검진이 주를 이루며 개별 환자에 따른 사회경제적, 결핵 관련 취약성을 확인하는 구체적인 지침은 마련되어 있지 않기 때문에 결핵관리 전담간호사에 따라 개별 결핵관리 요구도, 건강 문제와 행동을 확인하는 정도는 차이가 난다[4, 5].
결핵 환자 중 약 85%는 6개월의 약물치료로 성공적으로 치료될 수 있고[1], 약물복용과 같은 결핵 환자의 건강행위(health behavior)는 결핵치료의 성과를 좌우한다[6]. 건강행위는 건강을 유지, 회복, 증진하는 데 영향을 미치는 행동이나 활동, 습관을 말한다[7]. 이는 관찰 가능한 외적 행동뿐 아니라 측정 가능한 정신적 그리고 감정 상태까지를 포함하고, 넓게 볼 때 그러한 행동에 영향을 주는 사회 환경적 결정요인들과 결과까지를 일컫는다[8]. 보건 사업의 효과적인 운영을 위해서는 사업대상의 특징에 따라 건강행위 간의 연계성과 독립성을 동시에 고려하고 그 특성을 이해하는 것이 중요하다[9, 10].
Marra 등[11]은 결핵 환자의 건강행위를 식단 변화, 운동을 더 하는 것을 포함한 행동을 변화시킨 것과 결핵에 대한 지식을 가진 것으로 언급했다. Sutherland 등[12]은 결핵 진단과 치료를 준수하는 것으로, Hargreaves 등[13]은 치료준수와 금연을 건강행위라 하였으며 Abrams [14]는 결핵 환자의 위험한 건강행위로 부주의한 침 뱉기를 언급했다. 이처럼 건강행위는 결핵 환자의 치료에 있어 중요성이 인정되어 여러 연구에서 적용되었다. 그러나 결핵 환자의 건강행위가 어떤 속성으로 구성이 되어있는지, 그리고 그 속성을 포함하여 결핵 환자의 건강행위 개념을 명료화한 연구는 아직 이루어지지 않았다.
결핵 극복에 있어 결핵 환자 개인의 건강행위는 여전히 가장 중요하며[14], 보건의료 제공자인 간호사는 결핵 환자에게 의미 있는 건강행위를 확인하고 권유해야 한다. 그러나, 명확히 정립되어 있지 않은 결핵 환자의 건강행위 개념은 간호사가 결핵 환자의 건강행위와 관련된 사정을 정확하게 하지 못하고 필요한 중재를 제공할 수 없게 한다. 즉, 결핵 환자의 건강행위에 대한 원인, 속성, 결과 등을 명확히 하지 않고선 가치 있는 건강행위를 권장할 수 없다[15]. 따라서 결핵 환자의 건강행위 개념을 명료화하기 위한 심도 있는 고찰과 분석이 필요하다. 그리고 이를 통해 보건의료 제공자인 간호사는 결핵 환자의 건강행위에 대한 이해와 민감성 역량이 증진되어 결핵 환자에게 건강행위를 적극적으로 권장할 수 있을 것이다.
개념은 사회적 맥락에서 시간이 지남에 따라 끊임없이 변화하고 진화하는 특성을 가진다[16]. 개념분석은 그 개념이 가진 독특한 속성과 특성을 이해하고 명확히 함으로써 모호한 개념을 구체화할 뿐만 아니라 때로는 간호에 부적절하거나 과도하게 적용되는 개념을 명료화하는 데 도움이 된다[17]. 건강행위를 정의할 때는 영향요인의 통합적이고 동적인 측면을 고려하고 정교하고 종단적인 자료수집을 강조한다[18]. 또 건강행위에 영향을 미치는 다양한 부문 중 정책과 환경은 주요 결정요인으로 크게 강조된다[7]. 현재 결핵치료는 WHO의 결핵 퇴치전략 아래에 각 나라 수준에 부합한 목표와 전략 수행이 기본원칙이다[3]. 1993년 WHO는 결핵 긴급 상황 선언을 하였으나 이는 세계적으로 관심을 받지 못하였고, 이 시기의 결핵관리 프로그램에 사회문화적 요인과 환자는 충분히 고려되지 않았다[19]. WHO는 2000년 The Stop TB Strategy를 통해 각국에 결핵 관련 투자 증가와 직접복약확인(Directly Observed Therapy, DOT)을 실시할 것을 권고하였고 그 결과 평균 결핵치료 성공률이 향상되었지만, 결핵 신고율과 결핵치료의 질은 향상되지 않았다[20]. 초창기 DOT를 포함한 무료 결핵 진단과 약물치료를 시작으로 이후 추가 서비스의 확장, 지역사회기반 지원, 환자 중심 전략을 포함한 The End TB Strategy에 이르렀다[3, 21]. 이처럼 결핵관리 사업은 보건체계, 결핵관리 프로그램 구성과 운영 그리고 그 구성요소를 포함하고 있고 이는 결핵관리 전략에 따라 변화되었다[21]. 이런 결핵관리 사업의 변화는 결핵 환자의 치료 관련 행동에도 영향을 미친다[22]. Rodgers의 진화론적 방법(evolutionary method)은 사회적, 문화적, 학문적 또는 이론적 맥락 등에서 광범위한 자료수집, 귀납적 접근과 분석을 통해 개념의 본질을 탐구하길 강조한다. 이는 결핵 환자의 건강행위 개념의 역동적인 의미를 알아보기 위한 분석방법으로 적절하다고 판단된다[23, 24, 25]. 이에 본 연구에서는 결핵 환자의 건강행위에 대한 개념을 Rodgers의 진화론적 개념분석의 틀에 근거해 명확히 하고 건강행위에 초점을 맞춘 간호 요구도 확인과 제공을 위한 이론적 근거를 제시하고자한다.
본 연구의 목적은 Rodgers의 진화론적 개념분석 방법을 통해 결핵 환자의 건강행위 개념을 더 잘 이해하고 식별하기 위함으로 구체적인 목적은 다음과 같다.
• 결핵 환자의 건강행위 개념의 선행요소, 영향요인, 속성, 결과를 규명한다.
• 결핵 환자의 건강행위 개념의 대체 용어, 관련 용어를 규명한다.
• 결핵 환자의 건강행위 개념을 정의하고 가설을 제시한다.
본 연구는 Rodgers의 진화론적 개념분석 방법[23, 26]을 적용한 결핵 환자의 건강행위에 대한 개념분석 연구이다. Rodgers의 진화론적 개념분석 방법은 6단계로 제시되어 있으나 이는 순서에 따르지 않고 동시적이고 순환적인 상호작용의 과정이며 단계 5는 선택적으로 수행할 수 있다(Table 1).
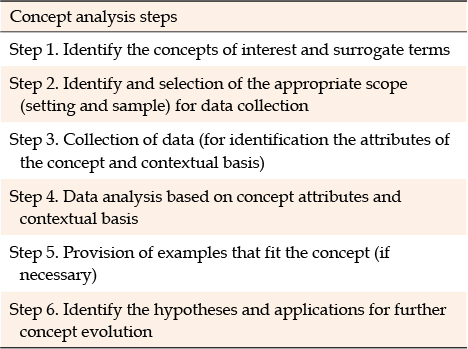
Table 1
Rodgers’ Evolutionary Concept Analysis Method
먼저 관심 개념을 정의하고 관련 문헌의 범위를 정했다[26]. 서로 다른 국가들의 건강행위 자료를 이용할 때 객관적 이해와 해석을 적용하기 위해서 공통된 양적 평가를 확인하는 것이 필요하며[3, 7], 이를 근거로 본 연구에서는 결핵 종식을 위해 전세계적으로 결핵관리 전략이 강화된[3] 2015년부터 2021년 4월까지 발표된 결핵의 맥락에서 건강행위에 관한 문헌을 분석에 포함했다. The End TB Strategy에는 기존 결핵관리 전략과 공통된 기준에 따른 결핵 결과 평가가 가능해졌다[3]. 문헌고찰을 위해 국외 문헌은 PubMed, ProQuest, Cumulative Index to Nursing and Allied Health Literature, Web of Science, Cochrane Library의 의과학 데이터베이스를 이용하였다. 국내 문헌은 국가과학기술정보센터(National Digital Science Library, NDSL), 국회도서관(National Assembly Library, NAL), 학술연구정보서비스(Research Information Sharing Service, RISS)의 검색 엔진을 이용하였다. 그 외 관련 문헌은 수동 검색을 통해 보완하였다[22]. ‘결핵 환자’ AND ‘건강행위’, ‘결핵 건강행위’, “tuberculosis patients” AND “health behavior”, “tuberculosis health behavior”를 사용해 관련 문헌을 검색하였다. 자료를 선택하는 과정에서 선정기준으로는 2015년부터 2021년 4월까지 출판된 논문, 영문과 한글로 발간되어 전문이 확인되는 논문, 논문심사위원의 심사를 거친 학술지를 포함했다. 제외 기준으로 건강행위에 대한 개념이나 특성이 설명되지 않은 논문, 소아 대상의 연구, 회색 문헌(잡지, 단순 건강정보 관련 논문 등)은 포함하지 않았다.
초기 검색 결과로 총 5,706개 문헌이 확인되었고 중복 문헌 제외, 선정기준 적용, 제목과 초록 검토를 통해 총 5,546건이 제외되어 160건의 문헌을 추출하였다[27]. Rodgers는 색인된 문헌이 방대한 경우, 난수표를 이용하는 등 확률표본추출법을 사용해 연구의 표본을 선택할 수 있다고 하였지만[14], 본 연구에서는 무작위 추출 시 제외조건에 해당하는 문헌이 다수 추출됨을 확인하여, 모든 문헌을 확인하였다. 160건 중 전문(full-text) 확인과 추가 수동 검색을 통해 최종적으로 69건의 문헌이 본 연구의 개념분석에 이용되었다(Figure 1, Appendix 1).
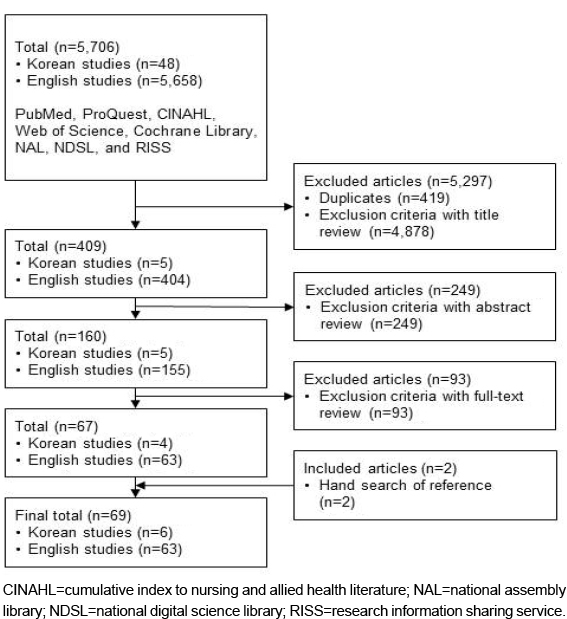
Figure 1
Flow of literature search and number of articles.
자료분석은 Rodgers가 제시한 진화론적 개념분석 단계[23, 26]를 순차적으로 진행함과 동시에 필요한 경우에는 각 단계를 순환, 반복적으로 수행하여 자료분석을 진행하였다. 다만, 자료수집이 완료된 후에 본격적인 자료분석을 시작하였다. 이는 수집과 분석의 동시 분석 시 발생할 수 있는 조급한 결론, 성급한 확신과 같은 오류를 예방하기 위함이었다[23]. 선정기준에 해당하는 문헌의 전문을 읽고, 그 후 개념의 맥락 속성, 선행요소, 결과, 대체 용어, 관련 용어에 초점을 맞춰 살펴봤다. 각 자료를 구분해 정리하고 그 후 비교해 유사성, 차이점, 시간이 지남에 따른 변화를 확인하면서 개념에 대한 일치, 합의되는 내용을 살펴봤다[23, 26].
연구자는 박사학위 과정에서 간호이론개발이라는 과목을 통해 개념분석에 대한 지식을 습득한 후, 다년간의 결핵 환자 간호를 통해 얻는 결핵 환자에 대한 이해를 바탕으로 결핵 환자의 건강행위에 대한 개념분석의 필요성을 인식하게 되었다. 개념분석 방법에 익숙해지기 위해 관련된 문헌들을 읽어보며 Rodgers의 진화론적 개념분석 방법을 이해하고 적용하기 위해 지속해서 노력하였다.
의약학 24편, 보건학 20편, 면역학 10편, 간호학 6편, 유전학 2편, 인문학 2편, 기타(학제 간, 공학, 법학, 재활의학, 약학) 각 1편의 학술 분야 연구논문이 분석되었다. 결핵 환자의 건강행위에 대해 직접적인 개념 정의를 내린 경우는 적었기 때문에, 대부분은 문헌에서 나타난 환자의 행동과 경험을 통해 개념을 분석하였다(Figure 2).
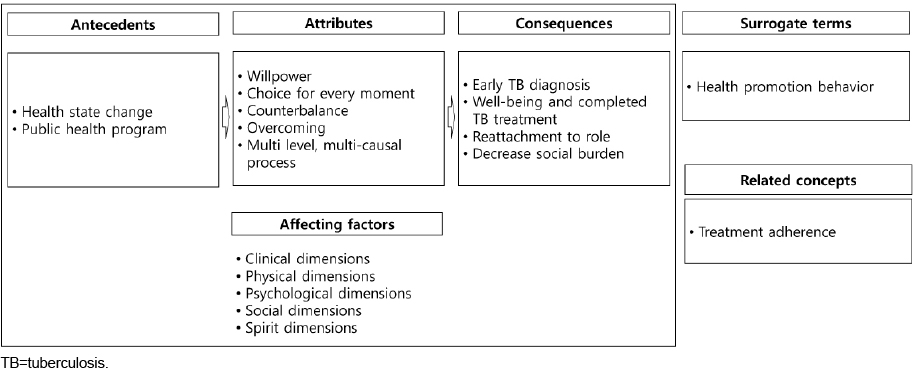
Figure 2
Concept’s components of the tuberculosis health behavior.
선행요소는 결핵 환자의 건강행위 이전의 상황, 사건이나 현상이다[23]. 결핵 환자의 건강행위는 결핵으로 인한 기침, 가래 등의 호흡기 증상이나 체중감소와 같은 건강상태 변화(health state change)가 발생함으로 일어난다[A5,A22,A50,A58]. 증상이나 건강상태 정도는 건강행위를 할 수 있는 동기를 제공한다[A58]. 때로는 지역 보건 프로그램(public health program)운영의 하나로 선별 검사를 통해 결핵 사례를 발견하기도 했다[A21,A60].
본 연구에서 선행요소, 속성, 결과를 포괄하며 결핵 환자의 건강행위에 영향을 미치는 요인들은 임상적(clinical dimensions), 신체적(physical dimensions), 심리적(psychological dimensions), 사회적(social dimensions), 영적(spirit dimensions) 차원이었다.
개념의 속성이란 그 개념에 대해 적절하게 특징지어 나타낼 수 있는 실질적인 정의를 의미한다[24]. 속성과 관련된 21개의 주제어에서 5개의 주요 속성이 도출되었다(Figure 3).
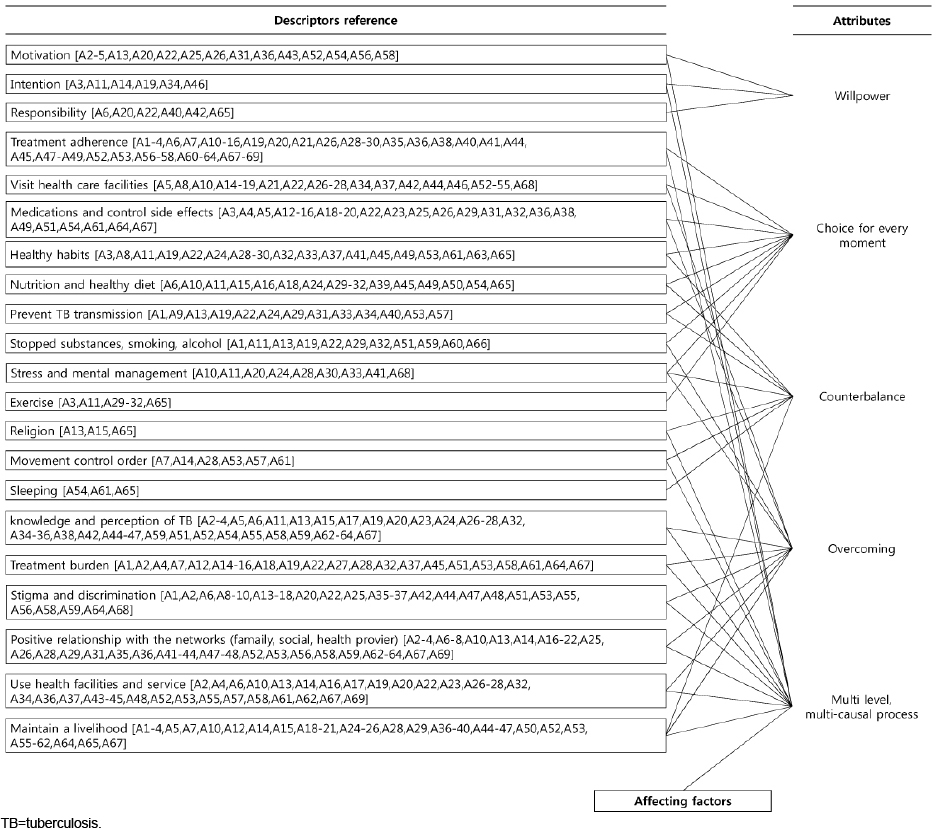
Figure 3
Flowchart of descriptors and attributes.
결핵 환자는 증상 호전을 위해[A3,A58], 치료받기 위해[A34], 치료를 유지하기 위해[A2,A31], 결핵과 관련된 정보를 찾기 위해[A22], 결핵 진단 이전처럼 역할을 수행하기 위해서[A25] 등의 이유로 행동하게 된다. 이런 의지(willpower)는 치료 제공자의 조언을 따르고, 자신을 스스로 격리하고, 결핵약을 계속 복용하는 것과 같은 행동을 변화시켜 긍정적인 사고와 자기 인식을 채택하게 된다[A13]. 결핵 환자의 의지는 개인의 내부에서뿐 아니라 타인을 위하는 마음이나[A34], 가족[A36], 보건의료 제공자, 정부의 격려 혹은 지원을 통해 가지게 되기도 한다[A16,A26,A55]. 결핵치료의 중요성[A36,A61]과 완치될 수 있다는 믿음[A13], 희망[A20]은 치유 욕구를 불러일으키고[A51,A58] 이는 삶의 의지와 건강행위로 연결된다[A15].
결핵 환자는 매일 행동을 반복적으로 선택한다[A57]. 치료지침을 준수하여 결핵약 복용하기, DOT 혹은 추구 검진을 받기 위해 기관에 방문하기, 결핵 전파 예방하기, 금연과 금주를 포함한 물질 사용 중단하기, 영양, 운동, 스트레스 및 정신 건강관리하기와 같은 행동을 언제, 어디서, 어떻게 수행할지에 대해 매번 결정하게 된다[A11]. 이러한 매번의 행동 선택(choice for every moment)은 습관화되어 종국에는 건강을 유지하고 증진하는 건강행위로 정착하게 된다[A29].
결핵 환자 개인은 변화된 상황과 몸에 대한 스트레스를 관리하기 위해 신앙을 이용하거나[A13,A15,A65], 치료와 일상 사이에서 균형을 추구하기 위해 수면이나 식습관, 생활 방식을 변화시킨다[A55,A61,A65]. 치료 참여를 최적화하기 위해 지역보건 프로그램은 결핵치료를 무료로 제공함으로써 통제와 환자의 자율성 사이에서 균형을 유지한다[A20]. 입원이나 격리를 통해 결핵 환자의 이동이 제한되거나[A2,A61,A68], 기침 예절과 올바른 가래 처리를 포함한 개인의 노력은 공중보건의 영역에서 결핵 전파를 방지하여 지역사회 내 결핵 유병률을 조정하였다.
질환은 부정적인 측면을 수반한다[27]. 결핵 환자에 대한 낙인이나 차별, 잘못된 지식과 인식은 환자로 하여금 결핵 진단을 거부하게 하고[A46], 질병에 대해 숨기거나 보건 시설에 방문하지 않게 한다[A42]. 그 밖에 DOT를 포함한 치료 지침 자체의 부담, 약물 부작용, 보건 시설을 이용하기 위해 내원하는 시간과 비용, 근로 중단을 포함한 사회경제적 부분, 정보를 요구하는 것, 결핵 서비스 운영의 질, 보건의료 제공자 자질과 그들과의 상호관계는 긴 치료 기간 동안 결핵 환자가 건강행위를 지속하기 위해 다루어야 할 부분이었다[A11]. 결핵 환자의 건강행위는 이런 문제 상황을 변경하거나 극복하여 더 좋은 미래를 위해 노력하는 과정이었다.
결핵은 결핵균에 의해 발생하는 질병이나 이를 포함하여 다양한 사회적 결정요소들이 영향을 준다[A15]. 마찬가지로 임상적, 신체적, 심리적, 사회적, 영적 차원은 결핵 환자의 건강행위에 영향을 주는 동시에 건강행위를 결정하는 수준이 된다. 요인의 다양성과 수준은 개인마다 다르며, 개인에 따라 언제, 어느 것이 중점이 되는지에 따라 특정 수준의 차원을 좀 더 강조한 건강행위를 할 수 있다[28]. 이러한 다수준 다요인 과정(multi level, multi-causal process)은 결핵치료가 끝날 때까지 상호작용하며 이뤄지기 때문에 진행 중인 과정임을 나타낸다.
결과는 결핵 환자의 건강행위로 인해 발생하는 사건이나 상황을 의미한다[23]. 본 연구에서는 결핵 조기 진단, 안녕(well-being)과 완전한 치료, 역할 복귀, 그리고 사회적 부담 감소가 결핵 환자의 건강행위로 인한 결과로 제시되었다.
결핵 진단과 치료가 가능한 보건 시설을 찾아 방문하는 결핵 환자의 건강행위는 결핵 조기 진단이라는 결과를 가져온다 [A34].
결핵 환자 건강행위는 생활 방식과 의식을 더 건강한 방향으로 변화시키면서 증상 완화뿐 아니라 삶의 여러 영역에서 증진에 기여한다[A13,A15,A24,A33,A61]. 금주, 건강한 생활 방식 채택, 건강에 관심을 가지고[A12,A65], 보건의료 제공자에게 필요한 정보를 요구할 수 있으며 건강 행동과 습관을 더 공고히 할 수 있다[A49]. 변화된 건강 상태와 치료 지침에 따라 업무에 적용하고[A61], 개인에 따라 외상 후 성장, 삶의 변화, 재구축(rebuilding oneself)이 이루어진다[A56]. 건강행위와 함께 결핵약 복용 효과로 기침 중단, 체중 증가, 객담검사 음성과 같은 결과가 나타나고 이를 유지하여 치료 기간이 끝난다면 치료 완료 판정을 받게 된다[A31].
결핵 환자의 초기 치료 단계에서는 결핵 전파 방지를 위해 일시적 격리 혹은 입원함으로써 가족을 포함한 다른 사람과 분리되게 된다[A57]. 그로 인해 일상적인 사회활동 수행에 제약이 발생하고 학생, 근로자, 양육자와 같은 사회적, 문화적으로 규정된 본래 역할을 수행할 수 없게 된다[A35,A53]. 결핵 증상이 악화되거나 전염성이 소실되지 않으면 원래의 사회적 역할에 돌아갈 수 없게 되고 이는 가정 내 소외, 일자리 소실, 사회적 소속감 저하, 고립으로 이어진다[A13-16,A58]. 치료준수를 포함한 결핵 환자의 건강행위는 결핵의 전염성을 소실시키고 중증 결핵으로의 전환을 막아 일상으로의 복귀를 유도해 본래의 역할을 할 수 있게 된다[A4].
결핵 환자의 건강행위로 지역사회 내 결핵 전파, 내성 결핵 발생을 예방할 수 있다[A12,A51]. 이는 새로운 결핵 환자나 중증 결핵 환자 치료에 소모되는 의료비를 줄일 수 있으며[A16], 치료비 외에도 교통비, 식료품, 거주비와 같은 부대 비용을 줄일 수 있다[A51]. 긍정적인 결핵치료에 참가했던 환자는 다른 환자들을 도와주는 사회적 지지 요소로의 역할도 수행할 수 있게 된다[A6]. 궁극적으로 이환율, 발생률, 사망률과 같은 결핵 관련 지표가 감소 되며 경제적 손실을 예방할 수 있다[A12,A15,A18,A51].
결핵 환자의 건강증진행위(health promotion behavior in patients with TB)란 더 높은 수준의 건강 상태를 이루기 위해 능동적으로 환경에 반응하는 행위로 영양, 운동, 휴식과 스트레스 관리, 대인관계, 건강관리, 자아실현이 포함된다[A30]. 결핵 환자의 건강증진행위는 본인의 건강에 책임감을 느끼고 주도적인 역할을 함으로써 생활양식 변화를 통해 자신의 건강과 안녕을 유지, 증진하는 행위이므로 대체 용어에 가장 적합하였다.
문헌에서 치료준수(treatment adherence)라는 용어가 사용됨을 볼 수 있었다. 대부분은 약물 준수(medication adherence)의 의미로 쓰였으며 미복용 3회 미만[A18], 90% 이상 복용[A63,A67], 중단 시 2주 이내 재복용[A69] 등 다양한 기준이 적용되었다. 처방된 치료를 위해 주어진 지침을 따르는 정도의 준수[A13]는 결핵 환자 건강행위의 일부 속성만을 포함하는 용어이다[A12].
다양한 건강행위 경험을 다루는 문헌의 수에 비해 건강행위에 대한 정의가 기술되어 있는 문헌은 드물었다. 그러나 건강행위의 정의를 기술하는 문헌들에서 의미하는 건강행위 개념들은 거의 다르지 않았다. 다만 결핵관리 프로그램이 이전의 보건의료 제공자 중심에서 현재 환자 중심의 패러다임으로 전환되고 강화되는 과정임을 고려할 때[A4,A20,A28,A38,A40,A43,A49], 간호학 분야에서는 환자의 주도성을 강조한 건강 증진[A29,A65], 자가간호(self-care)[A31,A54], 건강 관련 삶의 질[A31,A48]과 같은 용어의 사용 빈도가 최근 증가하였음을 알 수 있었다. 지역과 가정 내 전통적인 성 역할을 고려해 건강행위를 이해하려는 접근은 유전학 분야 문헌에서 두드러졌다[A35,A46].
공통으로 결핵 환자의 건강행위는 개인 수준의 측면을 넘어 국가의 정책적 특징, 의료 시스템과 치료 관행, 지역사회 인식 등 지역의 사회문화적 구성과 얽혀 있었다. 결핵 환자의 사회문화적 맥락을 이해하기 위해 다면적이고 포괄적인 접근은 필수적이고 이를 반영한 지역사회 기반 중재가 필요하다는 것에 의견을 같이하고 있었다.
결핵 환자의 건강행위는 결핵치료에 있어 중요하지만[14], 그 개념에 대한 정의가 아직 명확하지 않고 어떤 속성이 있는지 파악된 바가 없다. 이에 Rodgers의 진화론적 방법을 사용해 결핵 환자의 건강행위에 대해 개념을 명확히 하고 선행요소, 결과를 포함한 속성을 확인하고자 본 연구를 시도하였다.
본 연구에서 결핵 환자의 건강행위는 5개의 속성으로 확인되었고 이는 의지, 매 순간의 선택, 균형 찾기, 극복하기, 다수준다요인 과정이었다. 건강행위에 대한 연구는 건강증진에 중요하게 기여한다[7]. 건강증진 중재에서 이론의 사용은 중재 효과에 대한 이해를 높이기 위해 제안되며, 이론적 기틀을 고정하지 않고 근거기반 행위변화 요소와의 연결을 통해 이론적 구성을 변경하는 것을 허용한다[7]. 본 연구에서 결핵 환자는 자신이 처한 상황을 인지하고 이를 긍정적인 방향으로 극복하려는 의지를 갖고 삶의 균형을 찾기 위해 매 순간 건강행위를 선택하며, 이러한 과정은 임상적, 신체적, 심리적, 사회적, 영적 차원과 상호작용하며 이뤄진다는 속성이 건강행위의 개념으로 도출되었다. 이는 Pender의 건강증진모델(Health Promotion Model, HPM)와 유사하다. HPM에 따르면 개인은 성찰적 자기 인식을 할 수 있는 능력을 갖추고 있으며, 변화와 안전성 사이에서 개인적으로 수용할 수 있는 균형을 이루기 위해 노력한다. 또 개인 환경과 상호작용하며 행동 변화에 있어 인간, 환경, 상호작용의 재구성은 필수적이라 하였다[29]. 이에 추후 결핵 환자의 건강행위 중재연구 개발 시 이론적 근거로 HPM을 적용하는 것이 적절할 것으로 사료 된다.
결핵 환자의 건강행위 선행요소는 ‘건강 상태의 변화’, ‘공중보건 프로그램’으로 나타났다. 이는 본연구의 대상자인 결핵 환자가 되기 위해 질병을 진단받게 되는 이전의 상황으로서 도출됐다. 변화된 몸 상태와 증상 수준은 건강행위 속성인 ‘의지’, ‘균형찾기’와 밀접한 연관이 있다. 증상 호전을 위해 건강행위를 시작하고 이를 지속시키는 동기로 작용하지만[A3,A58], 일부는 증상의 호전을 치료 완료로 보고 건강행위를 조기 종료한다[A25,A51]. 하지만 증상이 재발하면 다시 건강의 평행선을 옮기기 위해 건강행위를 재시도한다. 따라서 간호사는 결핵 환자의 진단 시 증상을 확인하고 치료과정 중 증상의 예상 변화에 대해 결핵 환자에게 알릴 필요가 있다. 특히 무증상이나 검진 등을 통해 진단받은 환자의 치료 의지는 더 낮을 수 있기에[A11] 치료 유지 중요성에 대한 지속적인 환기가 제공되어야한다.
주제어 분석은 개념의 귀납적 해석을 가능하게 하고 순환적 해석 접근에 몰입하게 할 수 있다[27]. 본 연구에서는 주제어 분석을 통해 개념 속성 분석을 수행하였다. 본 연구에서 나타난 주제어는 Arakelyan 등[22]의 연구에서 도출된 결핵치료 관련 요인들과 유사해 결핵치료에 있어 건강행위의 중요성이 지지되었다.
본 연구의 첫 번째 속성인 ‘의지’는 동기, 의도, 책임감 주제어 분석을 통해 도출되었다. 만성질환자의 건강행위 실천을 위한 의지의 속성을 분석한 Lee와 Kim의 연구[30]에서, 의지에는 의도된 목표, 계획을 실행하는 자기효능감, 자기 조절이 있는 것으로 나타나 본 연구와 유사하면서도 일부 차이가 있었다. 일반 만성질환자와 달리 타인에게 전파가 가능한 결핵의 특성상 이를 예방하는 것을 포함한 도덕적 의무를 결핵 환자들은 가지고 있다[A6]. 특정 질환에 따라 의지가 발휘되는 배경은 다를 수 있으며, 간호사는 다른 만성질환과는 다른 결핵 환자의 특성을 유의하며 사정해야 할 필요가 있다.
두 번째 속성인 ‘매 순간의 선택’은 치료준수, 건강시설 방문, 약물복용과 부작용 조절, 건강 습관, 영양과 식이, 결핵 전파 예방 등의 주제어에서 도출되었다. 이는 Lisum 등[31]의 연구에서 나타난 결핵 환자의 치료준수 속성인 ‘개인행동’과 유사하다. 이런 행동들은 내부와 외부의 자극으로 인해 일어나기 때문에[31] 간호사가 결핵 환자의 건강행위에 영향을 미치는 개인적 요소들을 파악하는 것은 매우 중요하다. 본 연구에서 결핵 환자의 건강행위에 영향을 주는 요인에는 임상적, 신체적, 심리적, 영적, 사회적 차원이 있었다. 결핵치료 지침, 결핵치료 제공 보건 시설과 서비스 운영, 보건의료 제공자는 결핵 환자의 건강행위에 영향을 주는 임상적 차원이었다. 신체적 차원은 동반 질환, 중독을 포함한 기존 건강 상태로, 기저질환은 결핵치료와 면역과정에 영향을 주기 때문에 건강행위를 통해 함께 조절해야 하는 부분이었다[A15,A65]. 하지만 반드시 기저질환이 치료나 면역과정에 영향을 미치는 것은 아니었는데, Human Immunodeficiency Virus (HIV)나 Coronavirus Disease 2019 (COVID-19)는 진단되지 않았음에도 동시 감염에 대한 높은 두려움과 우려 같은 심리적 차원의 문제도 나타났다[A13,A53,A58]. 심리적 차원은 특히 결핵 환자 중재의 제언으로 주로 언급되어, 중요성은 인식하고 있으나 여전히 결핵관리 프로그램에서는 누락된 서비스 지원이었다[A10]. 최근 COVID-19 대유행은 결핵 환자와 보건의료 제공자의 대면 상호작용을 감소시켰고 전화를 포함한 비대면 원격진료와 결핵 환자가 자신을 돌보는 역할이 증가하였다[31]. 긍정적인 심리적 상태는 필요시에 의학적 조언을 구하고 처방된 치료 지침을 잘 따르는 것과 같이 건강행위에 긍정적인 영향을 미친다[A10]. 따라서 간호사는 의료나 환자 개별 상황에 따라 환자와 상호작용하는 방법을 적용해야 하며, 정기적인 면담이나 전화상담을 통해 주기적으로 결핵 환자의 심리상태를 확인하고 심리적 지지를 제공해줘야 한다.
결핵 환자는 현재 자신에게 어떤 어려움이 있는지, 어떤 것에 도전해야 하는지를 인식하고 이런 역경을 변화시키거나 ‘극복하기’ 위해 건강행위를 함으로써 노력하게 된다. 간호사는 결핵 환자가 건강행위를 수행하는데 어려움을 미치는 요인을 무엇으로 인지하고 있는지 사정해야 할 필요가 있으며 환자와 함께 극복목표를 설정하고 성과에 대해 피드백을 제공하는 것은 환자의 행동 변화 효과에 도움이 될 수 있을 것이다[7].
Lisum 등[31]의 연구에서는 결핵치료에 영향을 미치는 내부 및 외부 요인을 선행요소로 나타냈지만 본 연구에선 ‘다수준 다요인 과정’을 결핵 환자의 건강행위의 선행요소가 아닌 속성으로 분류됐다. 요인들은 계속 변화하면서 건강행위와 끊임없이 영향을 주고받기 때문에 사전에 발생하는 것이 아닌 건강행위 과정 내내 일어난다. 결국 결핵 환자는 다차원적인 요인들과 상호작용하여 건강행위를 결정하므로, 건강행위를 증진하고 질병을 예방할 수 있는 다양한 경로를 식별하는 것이 필요하다. Arakelyan 등[22]의 연구에서도 결핵치료는 여러 사회생태학적 수준에서 복잡하고 역동적인 상호작용이 일어나며 보건의료 제공자는 결핵 진단을 넘어 이를 인식하고 결핵 환자의 숨겨진 취약성을 확인해야 한다고 강조했다. 정책 관련자들도 이런 인식을 바탕으로 보건 사업으로서 건강행위를 장려하기 위해선 관련된 조건을 개선하는 정책을 수립해야 할 필요가 있다[28]. 따라서 본 연구결과에서 나타난 결핵 환자의 건강행위 개념은 환자 개개인에게만 국한된 것이 아닌 결핵 퇴치를 위한 이해관계자들 모두가 고려해야 하는 속성이라 사료된다.
본 연구의 결과로 나타난 결핵 환자의 건강행위 속성인 ‘의지’, ‘매 순간의 선택’, ‘균형 찾기’, ‘극복하기’, ‘다수준 다요인 과정’은 결핵 환자의 치료준수에 관한 개념분석 결과로 ‘개인 행동’, ‘관계’, ‘공유된 의사결정’, ‘상호참여’, ‘합의’라는 5가지 속성을 나타낸 Lisum 등[31]의 연구와는 차이가 있었다. 치료 준수는 보건의료 제공자와 환자 간의 치료 결정 과정이라는 맥락에서 나타나며[31], 본 연구의 건강행위는 치료준수를 포함한 치료 경험 과정이라는 확장된 맥락에 중점을 뒀기 때문이다. ‘맥락’은 다양한 환경에서 건강행위를 지원하거나 방해하는 방식을 조정하는 결정요인에 영향을 주기 때문에[7], 맥락에 따라 개념이 차이가 있음을 유념해야 할 필요가 있다.
Rodgers의 개념분석 방법의 의의인 시간과 맥락에 따른 개념의 변화를 알아보기 위해 사용된 용어를 살펴볼 필요가 있다. 대다수 문헌에서 ‘치료준수’를 사용했지만, 일부 문헌에서는 ‘환자 중심’이라는 단어를 사용하면서 장기간의 결핵치료에 보건 관리 프로그램을 따르는 정도가 아닌 환자가 적극적으로 참여하여 치료에 대한 환자의 결정에 우선권을 인식하고 있음을 반영했다[A40,A43]. 그러나 결핵 환자의 건강행위 속성으로 ‘환자 중심(patient self)’이 도출되지는 않았다. Rodgers의 진화론적 개념분석방법은 현 상태를 파악하는 수단으로 이용되기 때문에[23], ‘환자 중심’은 많은 연구에서 그 중요성이 강조되었기는 하나 현재 속성에 들어갈 만큼 공통된 행동으로 나타나지는 않았기 때문이다.
Kielmann 등[A28]은 환자 중심이라는 관점이 치료 결과를 온전히 환자의 책임으로 부당하게 지게 하지는 않아야 한다고 우려했다. 결핵균이 처음 증명된 19세기, 결핵은 미생물이 원인으로 발생하는 단일 요인 질병(mono-causal disease)임이 명백했다[32]. 국제적인 결핵 퇴치 운동으로 나라마다 결핵 관리 프로그램들을 운영하고 있지만 이런 결핵 관리 프로그램들은 의료 시설 기반의 중앙 집중식이었다[A2,A52,A67]. 결핵균에 초점이 맞춰진 관리는 결핵약을 사용한 치료에 집중되었다. 환자가 처해있는 상황은 고려되지 못한 채 세균 전파를 막기 위한 물리적인 격리로 환자를 고립시키고 DOT에 참여하게 했으며 환자의 순응과 비순응으로 그 결과를 바라보았다. 이는 특히 다양한 지역적, 문화적 특성이 산포되어 있는 나라에서 환자의 취약 요소를 명확히 평가하지 못한 채 일괄적이고 엄격한 치료 접근만을 제공하여 효과적인 결핵치료 참여로의 장벽에 직면했다[A2,A35]. 이러한 비판과 변화 필요성을 반영하듯 최근 문헌들에서는 의료 서비스 접근이나 서비스 제공 부분에서의 변화를 강조하고 있었다[A6,A44,A48,A53]. 지역사회 지도자를 교육하거나 활용[A46], 기존 치료사를 통한 관리[A4]는 민간치료사의 영향력이 높은 지역의 문화적 맥락에서 활용할 수 있는 서비스 제공 방법이 될 수 있을 것이다.
건강행위의 정의는 건강 결과와 연결된다[7]. 본 연구에서 결핵 환자의 결과(output)는 정해진 기간 안에 결핵균 검사가 음성이고 약물치료를 완료했는지로 판정내리는 기준[1]을 넘어서 결핵의 조기 진단, 안녕(well-being)과 역할 복귀, 사회적 부담 감소로 확대되었다. 이는 사회적 맥락에서 결핵 환자의 결과 평가를 반영한 것인데, 결핵은 치료를 완료하더라도 평생 재발의 위험이 있으며 재발 결핵은 발병률이 높은 국가에서 성인 결핵의 주요 원인이기도 하다[33]. 약물치료 이후에도 건강한 생활방식을 지속하는 것은 환자의 평상시 면역력을 유지 시켜 결핵 재발의 위험을 낮출 수 있을 것이다. 따라서 결핵 환자의 약물치료 종료 시점에 건강행위를 지속해서 수행할 수 있는지를 함께 측정하고 간호사는 증진이 필요한 건강행위를 권유함으로써 결핵의 재발과 그로 인한 사회적 부담을 줄일 수 있을 것이다.
본 연구는 결핵 환자의 건강행위 개념에 대한 중요성과 이해를 바탕으로 오늘날 결핵 환자의 건강행위 속성을 포함해 선행요소와 결과를 분석함으로써 간호사를 포함한 보건의료 제공자의 중재 접근, 보건 관리 프로그램 발전에 기초자료를 제공한다는 점에서 의의가 있다. 그러나 양적 평가가 가능해진 결핵 퇴치전략이 전 세계에 적용된 2015년 이후를 기준으로 제한된 데이터베이스에서의 검색과 영어와 한국어로 된 문헌만을 분석하였기 때문에 모든 문헌을 대표하지 못하고 충분한 시간적 흐름의 맥락이 반영되지 못했을 수 있으며 간호학적인 객관성을 완벽히 유지하지 못했다는 제한점이 있다.
본 연구는 Rodgers의 진화론적 개념분석 방법을 이용하여 결핵 환자의 건강행위 개념분석을 수행하였다. 연구를 통해 확인된 속성을 내포한 결핵 환자의 건강행위 개념의 정의는 ‘결핵으로 인해 변화된 다양한 상황에서 삶의 균형을 찾기 위하여 결핵 환자가 의지를 갖고 매번 수행하는 행동들로, 다양한 요인들과의 상호작용을 통해 결핵 환자에게 닥친 어려움을 극복하고 종국에는 개인과 사회에 긍정적인 결과를 끌어내는 행위’이다. 본 연구에서 도출된 결핵 환자의 건강행위 개념의 진화론적인 발달을 위한 가설은 다음과 같다. 첫째, 결핵 환자의 건강행위는 매번 선택해야 하고 이를 위해선 의지가 있어야 한다. 둘째, 결핵 환자는 균형을 찾는 것을 목표로 건강행위를 한다. 셋째, 결핵 환자는 다차원적 요인과 상호작용하며 건강행위를 수행한다. 연구결과에 따르면 진화적으로 결핵치료에 ‘환자 중심’ 접근에 대한 중요성이 상당히 높아졌다. 이는 결핵 환자가 건강행위를 수행할 수 있도록 다차원의 관점에서 환자를 평가하고 정보, 재정, 심리적 지원을 포함한 지역사회 기반의 포괄적 중재와 자질 있는 보건의료 제공자를 갖춰야 하며 약물 완료가 아닌 본래의 역할로 되돌아가고 건강생활을 유지하는 것까지를 고려해야 함을 나타낸다. 본 연구결과는 향후 간호교육 분야에서 간호사의 결핵 환자의 건강행위에 대한 이해와 민감성을 발달시키기 위한 교육 프로그램을 제시할 수 있다. 간호 연구 분야에서는 결핵 환자의 건강행위에 대한 이론을 구축하는데 기초적인 자료로 활용될 수 있다. 또 본 연구에서 확인된 속성을 반영한 새로운 결핵 환자의 건강행위 측정도구를 개발할 수 있을 것이다. 간호 실무 분야에서는 결핵 환자의 건강행위에 관심을 두는 간호사와 보건의료 제공자 간의 의사소통을 증가시킬 수 있다. 결핵관리사업에 핵심 인물인 간호사는 결핵 환자의 건강행위 이해 역량 증진을 통해 결핵 환자의 건강행위와 관련된 간호요구도와 그에 맞는 중재를 적용할 수 있을 것이며, 그 효과를 결과와 연계해 검증하는 연구를 제언한다.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - KH-J and LMK.
Data collection - KH-J and LMK.
Analysis and interpretation of the data - KH-J and LMK.
Drafting and critical revision of the manuscript - KH-J and LMK.
A1. Abraham GV, Muruganandham R, Ganapathy K, Dhamodharan ASR. Gaps in infection control practices of tuberculosis among the patients attending designated microscopy centre( DMC): mixed method study. Online Journal of Health & Allied Sciences. 2018;17(3):3.
A2. Aibana O, Dauria E, Kiriazova T, Makarenko O, Bachmaha M, Rybak N, et al. Patients' perspectives of tuberculosis treatment challenges and barriers to treatment adherence in Ukraine: a qualitative study. BMJ Open. 2020;10(1):e032027. https://doi.org/10.1136/bmjopen-
A3. Akeju OO, Wright SCD, Maja TM. Lived experience of patients on tuberculosis treatment in Tshwane, Gauteng Province. Health SA Gesondheid. 2017;22:259-67. https://doi.org/10.4102/hsag.v22i0.1012
A4. Alegria-Flores K, Weiner BJ, Wiesen CA, Lich KLH, Van Rie A, Paul JE, et al. Innovative approach to the design and evaluation of treatment adherence interventions for drug-resistant TB. The International Journal of Tuberculosis and Lung Disease. 2017;21(11):1160-6. https://doi.org/10.5588/ijtld.17.0296
A5. Almeida CP, Skupien EC, Silva DR. Health care seeking behavior and patient delay in tuberculosis diagnosis. Cadernos de Saude Publica. 2015;31(2):321-30. https://doi.org/10.1590/0102-
A6. Anthoney J, De Wildt G, Meza G, Skelton J, Newell I. Patients' perspectives on factors facilitating adherence to tuberculosis treatment in Iquitos, Peru: a qualitative study. BMC Health Services Research. 2021;21(1):345. https://doi.org/10.1186/s12913-
A7. Azizi N, Karimy M, Salahshour VN. Determinants of adherence to tuberculosis treatment in Iranian patients: application of health belief model. The Journal of Infection in Developing Countries. 2018;12(9):706-11. https://doi.org/10.3855/jidc.9653
A8. Barua M, Van Driel F, Jansen W. Tuberculosis and the sexual and reproductive lives of women in Bangladesh. PLoS ONE. 2018;13(7):e0201134. https://doi.org/10.1371/journal.pone.0201134
A9. Beser A, Bahar Z, Haney MO, Aydogdu NG, Gurkan KP, Arkan G, et al. Cultural attitudes of society towards tuberculosis patients: a qualitative study. Journal of Pakistan Medical Association. 2018;68(7):1060-4.
A10. Chandra M, Rana P, Chandra K, Arora VK. Tuberculosis-depression syndemic: a public health challenge. Indian Journal of Tuberculosis. 2019;66(1):197-202. https://doi.org/10.1016/j.ijtb.2019.02.007
A11. Chen Y, Tan D, Xu Y, Wang B, Li X, Cai X, et al. Effects of a HAPA-based multicomponent intervention to improve self-management precursors of older adults with tuberculosis: a community-based randomised controlled trial. Patient Education& Counseling. 2020;103(2):328-35. https://doi.org/10.1016/j.pec.2019.09.007
A12. Choi H, Chung H, Muntaner C, Lee M, Kim Y, Barry CE, et al. The impact of social conditions on patient adherence to pulmonary tuberculosis treatment. The International Journal of Tuberculosis and Lung Disease. 2016;20(7):948-54. https://doi.org/10.5588/ijtld.15.0759
A13. Choowong J, Tillgren P, Söderbäck M. Thai people living with tuberculosis and how they adhere to treatment: a grounded theory study. Nursing & Health Sciences. 2017;19(4):436-43. https://doi.org/10.1111/nhs.12362
A14. Craig GM, Zumla A. The social context of tuberculosis treatment in urban risk groups in the United Kingdom: a qualitative interview study. International Journal of Infectious Diseases. 2015;32:105-10. https://doi.org/10.1016/j.ijid.2015.01.007
A15. Da Silva RD, de Luna FDT, de Araújo AJ, Camelo ELS, Bertolozzi MR, Hino P, et al. Patients' perception regarding the influence of individual and social vulnerabilities on the adherence to tuberculosis treatment: a qualitative study. BMC Public Health. 2017;17(1):725. https://doi.org/10.1186/s12889-
A16. Deshmukh RD, Dhande DJ, Sachdeva KS, Sreenivas A, Kumar AM, Satyanarayana S, et al. Patient and provider reported reasons for lost to follow up in MDRTB treatment: a qualitative study from a drug resistant TB centre in India. PLoS ONE. 2015;10(8):e0135802. https://doi.org/10.1371/journal.pone.0135802
A17. Diefenbach-Elstob T, Plummer D, Dowi R, Wamagi S, Gula B, Siwaeya K, et al. The social determinants of tuberculosis treatment adherence in a remote region of Papua New Guinea. BMC Public Health. 2017;17(1):70. https://doi.org/10.1186/s12889-
A18. Gugssa Boru C, Shimels T, Bilal AI. Factors contributing to non-adherence with treatment among TB patients in Sodo Woreda, Gurage Zone, Southern Ethiopia: a qualitative study. Journal of Infection and Public Health. 2017;10(5):527-33. https://doi.org/10.1016/j.jiph.2016.11.018
A19. Gyimah FT, Dako-Gyeke P. Perspectives on TB patients' care and support: a qualitative study conducted in Accra Metropolis, Ghana. Globalization & Health. 2019;15(1):19. https://doi.org/10.1186/s12992-
A20. Horter S, Stringer B, Greig J, Amangeldiev A, Tillashaikhov MN, Parpieva N, et al. Where there is hope: a qualitative study examining patients' adherence to multi-drug resistant tuberculosis treatment in Karakalpakstan, Uzbekistan. BMC Infectious Diseases. 2016;16:362. https://doi.org/10.1186/s12879-
A21. Hussain T, Tripathy SS, Das S, Satapathy P, Das D, Thomas B, et al. Prevalence, risk factors and health seeking behaviour of pulmonary tuberculosis in four tribal dominated districts of Odisha: comparison with studies in other regions of India. PLoS ONE. 2020;15(4):e0227083. https://doi.org/10.1371/journal.pone.0227083
A22. Iribarren SJ, Rodriguez Y, Lin L, Chirico C, Discacciati V, Schnall R, et al. Converting and expanding a mobile support intervention: focus group and field-testing findings from individuals in active tuberculosis treatment. International Journal of Medical Informatics. 2020;136:104057. https://doi.org/10.1016/j.ijmedinf.2019.104057
A23. Jakasania A, Shringarpure K, Kapadia D, Sharma R, Mehta K, Prajapati A, et al. "Side effects--part of the package": a mixed methods approach to study adverse events among patients being programmatically treated for DR-TB in Gujarat, India. BMC Infectious Diseases. 2020;20(1):918. https://doi.org/10.21203/rs.3.rs-
A24. Jankowska-Polanska BK, Kamińska M, Uchmanowicz I, Rycombel A. Quality of life and health behaviours of patients with tuberculosis-sex differences. Pneumonologia i Alergologia Polska. 2015;83(4):256-65. https://doi.org/10.5603/PiAP.2015.0046
A25. Kastien-Hilka T, Abulfathi A, Rosenkranz B, Bennett B, Schwenkglenks M, Sinanovic E. Health-related quality of life and its association with medication adherence in active pulmonary tuberculosis-a systematic review of global literature with focus on South Africa. Health and Quality of Life Outcomes. 2016;14:42. https://doi.org/10.1186/s12955-
A26. Khan AU, Akhtar N, Madni MA, Tahir N, Rehman M, Raza A. Socio-economic constrains faced by TB patients that lead to non-compliance-a cross sectional study in Southern Punjab, Pakistan. Acta Poloniae Pharmaceutica. 2016;73(6):1659-64.
A27. Khan MS, Hutchison C, Coker RJ. Risk factors that may be driving the emergence of drug resistance in tuberculosis patients treated in Yangon, Myanmar. PLoS ONE. 2017;12(6): e0177999. https://doi.org/10.1371/journal.pone.0177999
A28. Kielmann K, Vidal N, Riekstina V, Krutikov M, van der Werf MJ, Biraua E, et al. "Treatment is of primary importance, and social assistance is secondary": a qualitative study on the organisation of tuberculosis (TB) care and patients' experience of starting and staying on TB treatment in Riga, Latvia. PLoS ONE. 2018;13(10):e0203937. https://doi.org/10.1371/journal.pone.0203937
A29. Kim HJ, Lee MK. The relationship between illness perception and health behaviors among patients with tuberculosis: mediating effects of self-efficacy and family support. Korean Journal of Adult Nursing. 2017;29(6):626-36. https://doi.org/10.7475/kjan.2017.29.6.626
A30. Kim SM, Seo NS. Factors influencing health promotion behavior in patients with pulmonary tuberculosis. Korea Academy Industrial Cooperation Society. 2019;20(4):129-36. https://doi.org/10.5762/KAIS.2019.20.4.129
A31. Lee HJ, Park JY. Self-care efficacy and health-related quality of life among patients on primary treatment for pulmonary tuberculosis: the mediating effects of self-care performance. Korean Journal of Adult Nursing. 2020;32(3):305-14. https://doi.org/10.7475/kjan.2020.32.3.305
A32. Lee IS, Jeon JH. The relationship between health locus of control in personality and self care behaviors of North Korean defectors. Legislation and Policy Studies. 2015;7(2):565-88. https://doi.org/10.22809/nars.2015.7.2.021
A33. Lee SR. Factors related to the health management in patients with pulmonary tuberculosis in Korea. Asia-pacific Journal of Multimedia Services Convergent with Art, Humanities, and Sociology. 2016;6(9):519-29. https://doi.org/10.35873/ajmahs.2016.6.9.048
A34. Li ZT, Yang SS, Zhang XX, Fisher EB, Tian BC, Sun XY. Complex relation among health belief model components in TB prevention and care. Public Health. 2015;129(7):907-15. https://doi.org/10.1016/j.puhe.2015.04.008
A35. Mason PH, Roy A, Spillane J, Singh P. Social, historical and cultural dimensions of tuberculosis. Journal of Biosocial Science. 2016;48(2):206-32. https://doi.org/10.1017/S0021932015000115
A36. McNally TW, de Wildt G, Meza G, Wiskin CMD. Improving outcomes for multi-drug-resistant tuberculosis in the Peruvian Amazon-a qualitative study exploring the experiences and perceptions of patients and healthcare professionals. BMC Health Services Research. 2019;19(1):594. https://doi.org/10.1186/s12913-
A37. Megerso A, Deyessa N, Jarso G, Worku A. Lived experiences of tuberculosis patients and their implications for early tuberculosis case identification and management in pastoralist community setting: a qualitative study in Borena zone, Oromia region of Ethiopia. BMC Health Services Research. 2020; 20(1):933. https://doi.org/10.1186/s12913-
A38. Min J, Chung C, Jung SS, Park HK, Lee SS, Lee KM. Understanding illness perception in pulmonary tuberculosis patients: one step towards patient-centered care. PLoS ONE. 2019;14(6):e0218106. https://doi.org/10.1371/journal.pone.0218106
A39. Mokti K, Isa Z, Abdul Manaf MR, Hayati F, Syed Abd Rahim SS. Nutritional burden in tuberculosis and inter-sectoral nutritional management for tuberculosis patients in Malaysia. Turkiye Klinikleri Journal of Medical Sciences. 2020;40(1): 83-95. https://doi.org/10.5336/medsci.2019-
A40. Moodley N, Saimen A, Zakhura N, Motau D, Setswe G, Charalambous S, et al. They are inconveniencing us'-exploring how gaps in patient education and patient centred approaches interfere with TB treatment adherence: perspectives from patients and clinicians in the free state province, South Africa. BMC Public Health. 2020;20(1):454. https://doi.org/10.1186/s12889-
A41. Nagarajan K, Das B. Exploratory, cross-sectional social network study to assess the influence of social networks on the care-seeking behaviour, treatment adherence and outcomes of patients with tuberculosis in Chennai, India: a study protocol. BMJ Open. 2019;9(5):e025699. https://doi.org/10.1136/bmjopen-
A42. Nyasulu P, Phiri F, Sikwese S, Chirwa T, Singini I, Banda HT, et al. Factors influencing delayed health care seeking among pulmonary tuberculosis suspects in rural communities in Ntcheu District, Malawi. Qualitative Health Research. 2016; 26(9):1275-88. https://doi.org/10.1177/1049732315588083
A43. O'Donnell MR, Daftary A, Frick M, Hirsch-Moverman Y, Amico KR, Senthilingam M, et al. Re-inventing adherence: toward a patient-centered model of care for drug-resistant tuberculosis and HIV. The International Journal of Tuberculosis and Lung Disease. 2016;20(4):430-4. https://doi.org/10.5588/ijtld.15.0360
A44. Oga-Omenka C, Wakdet L, Menzies D, Zarowsky C. A qualitative meta-synthesis of facilitators and barriers to tuberculosis diagnosis and treatment in Nigeria. BMC Public Health. 2021;21(1):279. https://doi.org/10.1186/s12889-
A45. Ogundele OA, Moodley D, Pillay AW, Seebregts CJ. An ontology for factors affecting tuberculosis treatment adherence behavior in sub-Saharan Africa. Patient Preference and Adherence. 2016;10:669-81. https://doi.org/10.2147/PPA.S96241
A46. Oshi DC, Oshi SN, Alobu IN, Ukwaja KN. Gender-related factors influencing women's health seeking for tuberculosis care in Ebonyi state, Nigeria. Journal of Biosocial Science. 2016;48(1):37-50. https://doi.org/10.1017/S0021932014000534
A47. Park S, George M, Choi JY. Quality of life in Korean tuberculosis patients: a longitudinal study. Public Health Nursing. 2020;37(2):198-205. https://doi.org/10.1111/phn.12691
A48. Rahayu SR, Fauzi L, Maharani C, Merzistya ANA, Firdhausy HS, Cahyani TD, et al. Patients' perspectives on tuberculosis services in Urban Area, Indonesia: an assessment using QUOTE TB Light. Turkish Journal of Computer and Mathematics Education. 2021;12(9):872-81.
A49. Ren J, Li Q, Zhang T, Li X, Zhang S, Wright J, et al. Perceptions of engagement in health care among patients with tuberculosis: a qualitative study. Patient Preference and Adherence. 2019;13:107-17. https://doi.org/10.2147/PPA.S191800
A50. Ren Z, Zhao F, Chen H, Hu D, Yu W, Xu X, et al. Nutritional intakes and associated factors among tuberculosis patients: a cross-sectional study in China. BMC Infectious Diseases. 2019;19(1):907. https://doi.org/10.1186/s12879-
A51. Sahile Z, Yared A, Kaba M. Patients' experiences and perceptions on associates of TB treatment adherence: a qualitative study on DOTS service in public health centers in Addis Ababa, Ethiopia. BMC Public Health. 2018;18(1):462. https://doi.org/10.1186/s12889-
A52. Samal J. Health seeking behaviour among tuberculosis patients in India: a systematic review. Journal of Clinical and Diagnostic Research. 2016;10(10):1-6. https://doi.org/10.7860/JCDR/2016/19678.8598
A53. Santos FLD, Souza LLL, Bruce ATI, Crispim JA, Arroyo LH, Ramos ACV, et al. Patients' perceptions regarding multidrug-resistant tuberculosis and barriers to seeking care in a priority city in Brazil during COVID-19 pandemic: a qualitative study. PLoS ONE. 2021;16(4):e0249822. https://doi.org/10.1371/journal.pone.0249822
A54. Yang SH, Jung EY, Yoo YS. Health literacy, knowledge and self-care behaviors in patients with pulmonary tuberculosis living in community. Journal of Korean Academy of Fundamentals of Nursing. 2020;27(1):1-11. https://doi.org/10.7739/jkafn.2020.27.1.1
A55. Shatil T, Khan N, Yunus FM, Chowdhury AS, Reza S, Islam S, et al. What constitutes health care seeking pathway of TB patients: a qualitative study in rural Bangladesh. Journal of Epidemiology and Global Health. 2019;9(4):300-8. https://doi.org/10.2991/jegh.k.190929.001
A56. Shiratani KN. Psychological changes and associated factors among patients with tuberculosis who received directly observed treatment short-course in metropolitan areas of Japan: quantitative and qualitative perspectives. BMC Public Health. 2019;19(1):1642. https://doi.org/10.1186/s12889-
A57. Silva DS, Dawson A, Upshur RE. Reciprocity and ethical tuberculosis treatment and control. Journal of Bioethical Inquiry. 2016;13(1):75-86. https://doi.org/10.1007/s11673-
A58. Skinner D, Claassens M. It's complicated: why do tuberculosis patients not initiate or stay adherent to treatment? a qualitative study from South Africa. BMC Infectious Diseases. 2016;16(1):712. https://doi.org/10.1186/s12879-
A59. Stosic M, Vukovic D, Babic D, Antonijevic G, Foley KL, Vujcic I, et al. Risk factors for multidrug-resistant tuberculosis among tuberculosis patients in Serbia: a case-control study. BMC Public Health. 2018;18(1):1114. https://doi.org/10.1186/s12889-
A60. Theron G, Peter J, Zijenah L, Chanda D, Mangu C, Clowes P, et al. Psychological distress and its relationship with non-adherence to TB treatment: a multicentre study. BMC Infectious Diseases. 2015;15:253. https://doi.org/10.1186/s12879-
A61. Ting NCH, El-Turk N, Chou MSH, Dobler CC. Patient-perceived treatment burden of tuberculosis treatment. PLoS ONE. 2020;15(10):e0241124. https://doi.org/10.1371/journal.pone.0241124
A62. Tola HH, Garmaroudi G, Shojaeizadeh D, Tol A, Yekaninejad MS, Ejeta LT, et al. The effect of psychosocial factors and patients' perception of tuberculosis treatment non-adherence in Addis Ababa, Ethiopia. Ethiopian Journal of Health Sciences. 2017;27(5):447-58. https://doi.org/10.4314/ejhs.v27i5.2
A63. Tola HH, Karimi M, Yekaninejad MS. Effects of sociodemographic characteristics and patients' health beliefs on tuberculosis treatment adherence in Ethiopia: a structural equation modelling approach. Infectious Diseases of Poverty. 2017;6(1):167. https://doi.org/10.1186/s40249-
A64. Tola HH, Tol A, Shojaeizadeh D, Garmaroudi G. Tuberculosis treatment non-adherence and lost to follow up among TB patients with or without HIV in developing countries: a systematic review. Iranian Journal of Public Health. 2015;44 (1):1-11.
A65. Tsai SL, Lai CL, Chi MC, Chen MY. Cigarette smoking and health-promoting behaviours among tuberculosis patients in rural areas. Journal of Clinical Nursing. 2016;25(17-18): 2511-9. https://doi.org/10.1111/jocn.13289
A66.Wessels J, Walsh CM, Nel M. Smoking habits and alcohol use of patients with tuberculosis at Standerton tuberculosis specialised hospital, Mpumalanga, South Africa. Health SA Gesondheid. 2019;24:1146. https://doi.org/10.4102/hsag.v24i0.1146
A67.Woimo TT, Yimer WK, Bati T, Gesesew HA. The prevalence and factors associated for anti-tuberculosis treatment non-adherence among pulmonary tuberculosis patients in public health care facilities in South Ethiopia: a cross-sectional study. BMC Public Health. 2017;17(1):269. https://doi.org/10.1186/s12889-
A68.Woith WM, Rappleyea ML. Emotional representation of tuberculosis with stigma, treatment delay, and medication adherence in Russia. Journal of Health Psychology. 2016;21(5): 770-80. https://doi.org/10.1177/1359105314538349
A69. Yin J, Wang X, Zhou L, Wei X. The relationship between social support, treatment interruption and treatment outcome in patients with multidrug-resistant tuberculosis in China: a mixed-methods study. Tropical Medicine & International Health. 2018;23(6):668-77. https://doi.org/10.1111/tmi.13066
 E-SUBMISSION
E-SUBMISSION