
Purpose
The treatment of chronic kidney disease aims to delay dialysis and prevent progression to end-stage health complications. This study aimed to validate the Korean version of the Chronic Kidney Disease Self-Care (CKDSC-K) scale, which is used to measure self-care behaviors in patients with chronic kidney disease.
Methods Data from 285 participants were collected between August and November 2020. Validity was assessed in terms of content, construct, and concurrence through the content validity index and exploratory and confirmatory factor analyses. The reliability of the CKDSC-K was examined using internal consistency.
Results The final instrument consisted of 15 items across five factors (medication adherence, diet control, exercise, smoking behaviors, and blood pressure monitoring). The content validity index of the CKDSC-K was ≥.80. Confirmatory factor analysis indicated that factor loadings for the five factors ranged from .41 to .99, which explains the total variance of 75.3%. The internal reliability of the instrument was .81.
Conclusion The CKDSC-K scale has demonstrated acceptable reliability and validity and can be utilized to assess self-care behaviours in patients with chronic kidney disease. Additional research is recommended to expand the psychometric evaluation of the CKDSC-K.
The treatment of chronic kidney disease aims to delay dialysis and prevent progression to end-stage health complications. This study aimed to validate the Korean version of the Chronic Kidney Disease Self-Care (CKDSC-K) scale, which is used to measure self-care behaviors in patients with chronic kidney disease.
Data from 285 participants were collected between August and November 2020. Validity was assessed in terms of content, construct, and concurrence through the content validity index and exploratory and confirmatory factor analyses. The reliability of the CKDSC-K was examined using internal consistency.
The final instrument consisted of 15 items across five factors (medication adherence, diet control, exercise, smoking behaviors, and blood pressure monitoring). The content validity index of the CKDSC-K was ≥.80. Confirmatory factor analysis indicated that factor loadings for the five factors ranged from .41 to .99, which explains the total variance of 75.3%. The internal reliability of the instrument was .81.
The CKDSC-K scale has demonstrated acceptable reliability and validity and can be utilized to assess self-care behaviours in patients with chronic kidney disease. Additional research is recommended to expand the psychometric evaluation of the CKDSC-K.
The global prevalence of Chronic Kidney Disease (CKD) has been consistently increasing with population aging and increased prevalence of chronic diseases such as hypertension, diabetes, and obesity. The reported worldwide prevalence of CKD is approximately 13.4% (11.7~15.1%) [1]. According to the CKD Surveillance System, the prevalence of CKD among those in their 30s has increased from 13.2% to 14.4% over the last decade and is predicted to reach 16.7% by 2030 [2]. The rising impact of CKD has been globally recognized as a serious public health problem with high medical expenses combined with a higher risk of end-stage CKD as well as comorbidities, including health complications and mortality [3, 4].
The optimal treatment of CKD plays a major role in disease management; however, since patients with CKD cannot expect full recovery, lifelong disease management is crucial [5]. Therefore, patients with CKD need to go beyond simply adhering to the treatment regimens prescribed by their physicians. They are required to directly participate in their treatment process and assume health maintenance responsibilities by engaging in self-care activities such as making healthy lifestyle changes and practicing health behaviors [6]. Consistent and effective self-care is important because patients at the pre-dialysis CKD stage are at an increased risk of health complications and accelerated progression to end-stage CKD [7].
The terms "self-care" and "self-management" have been used interchangeably in literature pertaining to CKD. Although there is no clear agreement on the definition, self-care refers to the activities involved in self-management [5, 8, 9, 10]. Self-care is defined as activities performed by people to maintain and improve their health via self-maintenance, monitoring, and management [11]. The World Health Organization (WHO) refers to self-care as an effective approach to improving the health status of chronically ill patients, and the first step is assessing one's knowledge, beliefs, and behaviors [12]. To provide individualized care to patients, it is essential to assess areas of self-care vital for patients with CKD, set appropriate goals, and provide relevant information and training [13].
Unlike other chronic diseases, patients with CKD are often diagnosed with multiple chronic diseases, including diabetes and hypertension, making self-care more complicated [14]. Although it is recommended that patients with CKD focus on treatment regimens and self-care behaviors based on the CKD stage, there are common self-care behaviors that all CKD patients should adhere to. Despite the importance of self-care behaviors in CKD [6, 9, 10, 11, 13], the self-care tools developed to date mainly target pre-dialysis [15] and dialysis patients with end-stage renal disease [16, 17, 18, 19], wherein various self-care activities such as diet and exercise [16, 19, 20], medication, and blood pressure monitoring [15] are measured together, thus, making it difficult to identify problematic self-care behaviors and develop individualized care plans. Therefore, these domains are not suitable for assessing individual self-care behaviours in patients with CKD at all stages.
In order to bridge this gap in existing research, researchers at Kaohsiung Medical University, Taiwan, utilized an extensive literature review and clinical experience to develop the Chronic Kidney Disease Self-Care (CKDSC) scale consisting of 16 items across five domains assessing self-care behaviors in patients with CKD at all stages of the disease. The five factors of the CKDSC scale are conceptual frameworks for measurement based on literature reviews on the self-care behaviors of CKD patients and the clinical experiences of nephrologists [21]. The CKDSC scale is not limited to any particular ethnicity or culture, type of dialysis, or CKD stage, and its validity has been verified in China and Taiwan [21, 22]. The current study aimed to develop the Korean version of the CKDSC (CKDSC-K) by translating the original version and verifying its validity.
The current methodological study verified the validity and reliability of the CKDSC-K for assessing self-care behaviors in patients with CKD.
Of the patients who visited the outpatient nephrology department and Hemodialysis (HD) room at a single university hospital in D city, adult patients diagnosed with CKD at all stages were selected by convenience sampling. Patients in the predialysis stage of CKD and those on peritoneal dialysis were informed of the study purpose and method during a regular monthly visit to the nephrology department. Patients on HD were provided with the same information on the day of HD. All the participants were asked to complete a questionnaire after consenting to participate in the study. Permission for data collection was obtained from the director of the nephrology department. Data were collected from July 25, 2020, to December 2, 2020, by two nurses who worked in the nephrology department.
Exploratory Factor Analysis (EFA) and Confirmatory Factor Analysis (CFA) were conducted to ensure the construct validity of the scale. The target sample size was determined to be 5~10 times the number of items on the scale or to include at least 100 samples, considering the number of samples required for the factor analysis [23]. After excluding 15 questionnaires with insufficient responses from a total of 285 collected questionnaires, 139 questionnaires were used in the EFA and 131 in the CFA. Because the number of items in the CKDSC was 16, a sufficient number of samples was secured for data analysis.
Sociodemographic characteristics such as sex, age, Body Mass Index (BMI)(kg/m2), marital status, and education were collected. For disease-related characteristics, the CKD stage, duration of CKD diagnosis, number of comorbid conditions, and smoking behavior were investigated.
The CKDSC consists of 16 items assessing self-care behaviors in patients with CKD [21, 22]. The 16 items comprised five items on medication adherence, four on diet control, three on exercise, two on smoking behavior, and two on blood pressure monitoring. Each item was scored on a five-point Likert scale (never=1, rarely=2, sometimes=3, often=4, and always=5), including six inverse items. Higher scores indicate higher levels of self-care. At the time of the development of the scale, its Cronbach's α was.83. In addition, Cronbach's α was .83 for medication adherence,.83 for diet control, .94 for exercise, .81 for smoking behavior, and .87 for blood pressure monitoring.
The translation guidelines of instruments or scales used in this study were based on Sousa and Rojjanasrirat's guidelines [24]. Permission to translate and statistically validate the original scale was obtained from the developers of the CKDSC via email. The Chinese and English versions of the scale were available for translation and validation. A clinical practitioner with a nursing degree from an English-speaking country and a researcher with nursing experience and fluency in English independently translated the scale. Once the forward translation of the English version was completed, the two researchers compared their work and made the necessary revisions.
Two nursing professors with clinical experience and nursing degrees from an English-speaking country independently back-translated the Korean version of the scale and revised the translation by comparing their work. A bilingual (Korean and Chinese) nursing major compared the back-translated version of the scale with the original Chinese version to determine the accuracy of the translation.
The face validity of the translated scale was assessed using the Content Validity Index (CVI). A group of experts rated the relevance of each item to the self-care behaviors of patients with CKD on a 4-point Likert scale. Responses of 4 (very relevant) and 3 (relevant) were scored as 1, and the rest were scored as 0. Feedback regarding the clarity and cultural suitability of the expression used for each item was obtained during meetings, and revisions were made as needed. A total of ten experts, including four nurses with over 15 years of clinical experience specializing in kidney failure management and HD, two nephrologists, and four nursing professors, participated in the validation process. To clarify the Korean translation, the translation of "myself" in the Medication Adherence factor was expressed as "freely", and the word "monitor" in the Blood Pressure Monitoring factor was written as "check". The item-level CVI and scale-level CVI of the scale were >.80, exceeding the cutoff value of .78 [25].
A pilot test was performed on 30 patients, including eight patients with a CKD diagnosis duration of <3 years, nine patients with a CKD diagnosis duration of ≥3 years and <5 years, and 13 patients with a CKD diagnosis duration of ≥5 years. The results of the pilot survey were not included in the CKDSC test. A researcher in charge of data collection asked the participants whether the meaning of an item was clear and collected their opinions regarding unclear expressions and difficulty in understanding an item or term. Participants commonly reported feeling confused when answering the direct translation of the item, "I do not smoke every day", since Korean and English use the opposite logic to answer a negative question. Accordingly, the sentence was revised to "I smoke every day".
The data were analyzed using SPSS-WIN Version 26.0 and AMOS Version 26.0 (IBM., Armonk, NY, USA). Sociodemographic characteristics and measurement variables were expressed as means, standard deviations, real numbers, and percentages.
For the item analysis, the mean, deviation, and normality (skewness and kurtosis) were determined. An Item-Total Correlation (ITC) coefficient was calculated to determine whether a factor analysis could be performed (the number of items with corrected ITC coefficients ≤.30 shall not exceed half the total number of items) [26] and to determine the contribution of each item (ITC≥|.30|) [27]. Following the correlation and item analyses to verify the construct validity, EFA and CFA were performed. Approximately half of the participants were randomly sampled (n=139) using SPSS, and principal component analysis and EFA were performed using Varimax. CFA was performed on the remaining data set (n=131) using AMOS to determine the model fit. The fit indices used for the model fit for the CFA were χ2(p) (p<.05), normed χ2(χ2/df) ≤3, Goodness of Fit Index (GFI) ≥0.80, Adjusted GFI (AGFI) ≥0.80, Normed Fit Index (NFI) ≥0.90, Comparative Fit Index (CFI) ≥0.90, Root Mean square Residual (RMR) ≤0.05, and Root Mean Squared Error of Approximation (RMSEA) ≤0.10 [28, 29]. The correlations between different factors were assessed using ITC coefficients, and the contribution of each factor was determined by calculating the correlation coefficient between the score of each factor and the total score. Convergent validity was assessed using factor loading ≥.40, Composite Construct Reliability (CCR), and Average Variance Extracted (AVE) [27, 28]. For reliability, Cronbach's α was calculated to measure the internal consistency.
To protect the privacy of participants, data collection commenced only after receiving approval from the institutional review board (1041078-202012-HR-378-01). Participants were informed about the purpose of the study, method of participation, principle of voluntary participation and withdrawal, and anonymity and confidentiality in the process of data collection and processing. Only participants who voluntarily signed an informed consent form were included in the study. Data without any personally identifiable information collected from the anonymous self-report questionnaires were coded and entered into a database. Participants were compensated for their participation.
Table 1 presents the general and disease-related characteristics of the EFA and CFA groups. The mean age of the participants was 57.14 years, and 54.7% were men. The mean BMI was 23.93 kg/m2. The duration of CKD diagnosis was <3 years in 113 participants (41.9%), ≥3 years and <5 years in 53 participants (19.6%), and ≥5 years in 104 participants (38.5%). The mean duration of the CKD diagnosis was 4.72 years. Most participants had two to three comorbid conditions. Of the total participants, 46 (17.0%) were previous smokers and 27 (10.0%) were current smokers. The homogeneity of the above characteristics was confirmed between the EFA and CFA groups.
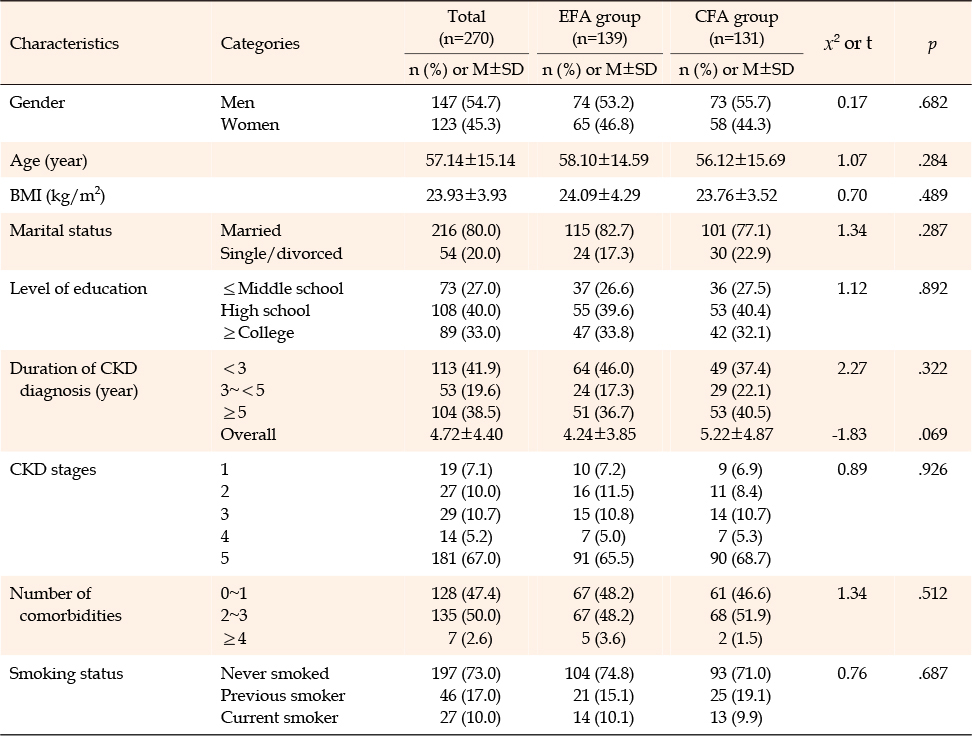
Table 1
General Characteristics of Participants (N=270)
The scores, skewness (≤±3.00), and kurtosis (≤±8.00) of each of the 16 items were examined to determine the normality. The kurtosis for item 5, "I sometimes changed the dose of my medication", was 18.24, and its contribution was .24 based on the ITC coefficient. Because the contribution was <.30 [30], the item was removed. After re-calculating the ITC coefficients for the remaining 15 items, the ITC coefficient for item 13, "I smoke every day" was found to be .23. Although the ITC coefficient was <.30, this item was considered essential since it assesses the smoking status of HD patients. Since the number of items with an ITC coefficient ≤.30 did not exceed half the total number of items, indicating that factor analysis could be performed [26], Item 13 was retained. The ITC coefficients for the other items were .30~.71 (Table 2).
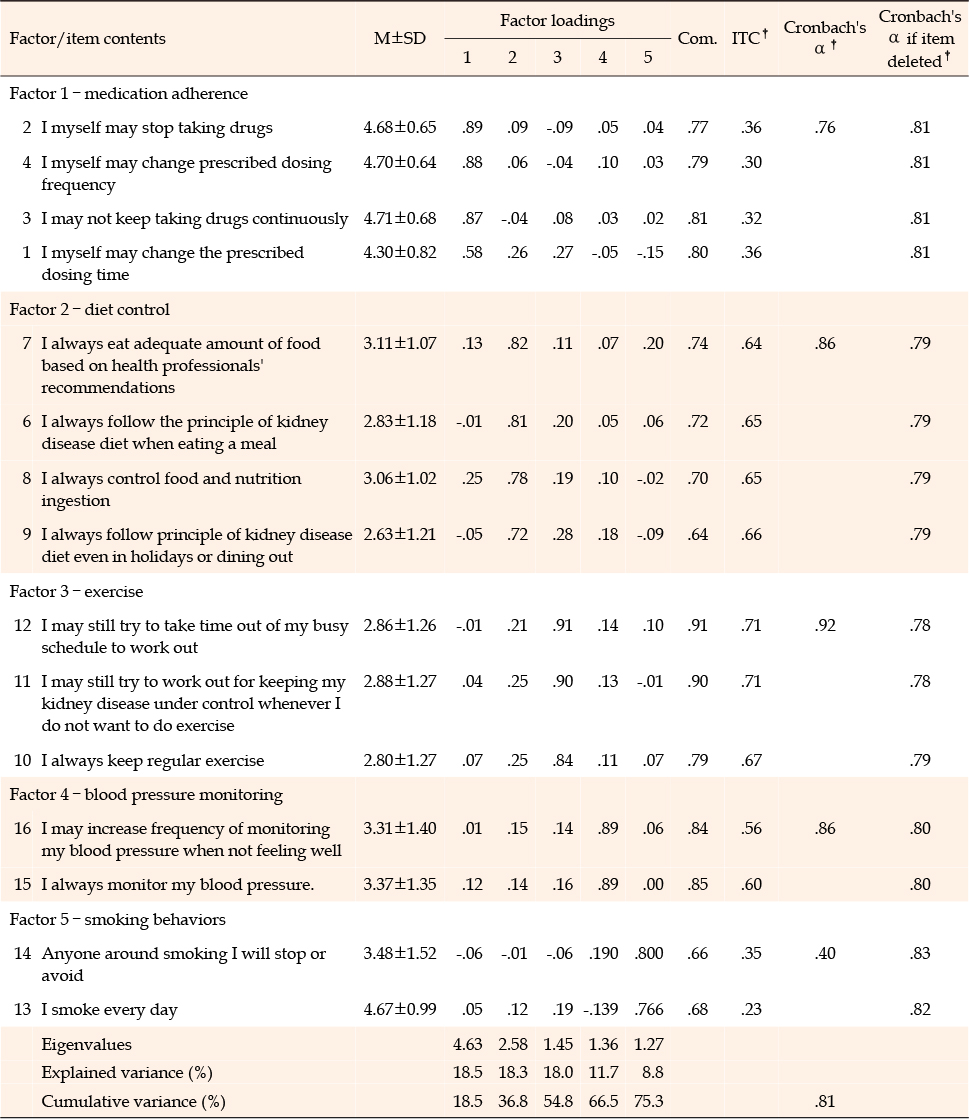
Table 2
Item Analysis and Exploratory Factor Analysis of CKDSC–K (N=139)
A Kaiser-Meyer-Olkin (KMO) value of .77 and a χ2 value of 1,051.01 (p<.001) were obtained for the 15 items in the EFA and Bartlett's Test of Sphericity, respectively, indicating that the data were suitable for factor analysis. Principal component analysis was performed using Varimax, in which the five factors identical to those in the original scale were extracted. Communality was ≤.50 and the factor loading was ≥.60 for all 15 items. The number of factors was set to five based on a scree plot, eigenvalues, explained variance, and cumulative explained variance. The five factors had eigenvalues of ≥1.00. The explained variance and cumulative explained variance were 8.8~18.5% and 75.3%, respectively (Table 2).
In the CFA, the factor loadings for the 15 items were.41~.99. All criteria for model fitness were satisfied: χ2 (p)=108.21 (.020), degree of freedom (df)=80, χ2/df=1.35, Goodness of Fit Index (GFI)=.90, Adjusted Goodness of Fit Index (AGFI)=.85, Normed Fit Index (NFI)=.89, Comparative Fit Index (CFI)=.97, Root Mean-square Residual (RMR)=.05, and Root Mean Square Error of Approximation (RMSEA)=.05. Although the AVE and CCR of factor 4 (smoking behavior) were .23 and .36, respectively, discriminant validity was established for factor 4 since the correlation coefficients between variables were smaller than the square root of the AVE value (Table 3).
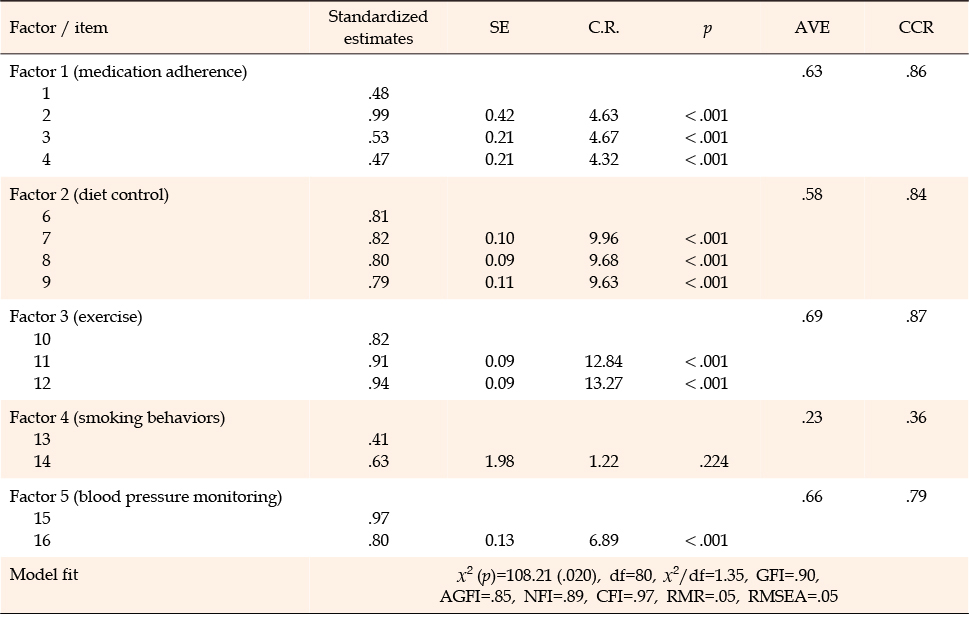
Table 3
Confirmatory Factor Analysis of CKDSC–K (N=131)
After removing item 5 from the CKDSC-K based on the results of the internal consistency test, Cronbach's α for the final instrument comprising 15 items was .81. Cronbach's α was .86 for diet control, .76 for medication adherence,.92 for exercise, .86 for blood pressure monitoring, and .40 for smoking behavior. The CKDSC-K showed the lowest reliability for smoking behavior.
The CKDSC-K scale was systematically developed in this study through forward and backward translation, expert CVI assessment, pilot study, cultural adaptation via cognitive debriefing, statistical validation, and finalization steps following guidelines on the translation, adoption, and validation of scales used in multicultural medical research in order to verify its validity and reliability [24].
In the item analysis, item 5, "I myself may change prescribed drug dosage", in the drug adherence domain, had a kurtosis of 18.24, indicating a non-normal distribution. The score for item 5 was 4.83, which was higher than previously reported scores of 4.65 and 4.61, indicating highly skewed responses [21, 22]. In the ITC analysis, the ITC coefficient (r) for item 5 was .24, not meeting the ≥.30 criterion [27]. Therefore, item 5 was removed from the scale. As response bias or ceiling effect may have occurred because the survey was conducted within a hospital, future studies using an anonymous online survey are suggested.
In addition, the construct validity and concurrent validity of the CKDSC-K were assessed. An EFA was performed on a scale with 15 items after removing item 5. The same five factors were extracted as those in the original scale. The variance explained by the items was evenly distributed between 8.8% and 18.5%. The cumulative explained variance was found to be relatively high (75.3 %). These values are close to the variance explained by each item and the cumulative variance explained (75.0%) was reported at the time of the scale's development [21]. In the CFA, Factor 4 in the smoking behavior domain had an AVE of .23 and CCR of .36, not satisfying the requirement for convergent validity [28, 29], although satisfying the criteria for discriminant validity. Thus, the scale is considered valid.
In the internal consistency assessment performed to verify reliability, Cronbach's α for factors 1 to 4 of the CKDSC-K was higher than .76. Cronbach's α for the smoking behavior domain was .40, lower than Cronbach's α of the same domain (.87) and the cut-off value (.70) in the original version [31]; therefore, reliability was not established for the smoking behavior domain. Of the two items in the smoking behavior domain, item 13 "I do not smoke every day" had an ITC of .23, indicating a low contribution to the scale but was not removed as it was deemed essential. This item was the most extensively discussed during the cognitive debriefing (refer to Section 2.4.3) and meetings. In the pilot test, participants tended to provide the opposite response to negative questions. This error was reduced by rewording the items into positive sentences. However, directly translating the English term "every day" to stay faithful to the original text resulted in a situation where participants who were intermittent smokers responded with a "no" to an item asking whether they smoked every day. The fact that the score of the item in question, which was 3.51 in a previous study, was 4.67 in this study, may indicate significance. Thus, it is necessary to examine the results of the CFA and internal consistency analysis after removing the word, "every day", and rewriting the item as "I currently smoke". Although direct comparison with previous results was difficult since previous studies have not reported the percentage of smokers [21, 22], only 10.0% of the participants in this study were current smokers, requiring reanalysis using data with more smokers. An additional analysis of self-care scores revealed significantly lower self-care scores for smokers than for those who used to smoke or those who never smoked, indicating that the smoking behavior domain and items adequately assess smoking-related self-care.
The average CKDSC score of the participants in this study was 3.56, lower than previously reported scores of 3.84 and 3.88 [21, 22]. Of the five domains (medication adherence, diet control, exercise, smoking behavior, and blood pressure monitoring), the diet domain had the largest score difference from previously reported scores. This may be because 67.0% of the participants in this study had stage 5 CKD, as opposed to only 22.3% and 24.7% in previous studies [21, 22]. A low-sodium diet with a limited intake of spicy or salty foods, as well as a controlled intake of water, is recommended for patients with CKD. A typical Korean diet includes salty or spicy soups and broths that contain a large amount of water. Thus, limiting water intake is difficult for Korean patients with CKD, who reported diet control as the biggest challenge in adhering to a treatment regimen because of deep-rooted dietary habits despite receiving diet education [15]. The items in the diet control and exercise domains of the CKDSC use adverbs of frequency such as "always" to assess self-care behaviors. Although using adverbs of frequency is a valid approach to assessing self-care behaviors given the importance of consistency in self-care behaviors, it is necessary to revise the CKDSC such that it uses precise frequencies instead of subjective terms, such as "never", "sometimes", and "often". In other words, adverbs of frequency must be replaced with exact frequencies after establishing linguistic, cultural, functional, and metric equivalence to confirm previous results [32].
The current study is meaningful in that it has developed a scale that helps not only HD patients but also patients with CKD to recognize the importance of self-care behaviors before undergoing HD so that they can self-assess and self-manage their self-care behaviors rather than having them assessed by a healthcare provider. However, since the participants were selected by convenience sampling from a single medical facility and the validity of the smoking domain of the instrument was lacking, additional verification and caution are required in interpreting the results of this study. Additionally, the impact of comorbidities such as diabetes and the duration of CKD diagnosis on self-care behaviors cannot be disregarded.
The CKDSC-K scale developed in the current study can be used to assess and monitor self-care behavior among patients with CKD at all stages of the disease. The CKDSC-K is a simple assessment tool that comprises 15 concise items that cover five essential self-care domains and can be completed within a short duration. Thus, it is highly likely to be used in various clinical settings. Based on the results, some robust recommendations for future research are suggested. First, repeated studies should recruit patients with CKD from several hospitals and data should be collected anonymously to avoid response bias. Second, a validation study targeting the smoker group is recommended to test the reliability and validity of the smoking factor of CKDSC-K. Although it is important to avoid changing the composition of the original scale or distorting the meanings of questions, it is important to repeatedly verify the validity and reliability of domains such as diet control-which is recognized as the most important aspect of CKD management-after ensuring functional and metric equivalence of the scale by tailoring it to the Korean cultural context.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - SYH and AJ-W.
Data collection - SYH.
Analysis and interpretation of the data - SYH, JH-Y and AJ-W.
Drafting and critical revision of the manuscript - SYH, JH-Y and AJ-W.
 E-SUBMISSION
E-SUBMISSION