
Purpose
This study aimed to compare the health expenditure and unmet health care needs and factors associated with these, in single-person households pre- and post-baby boomer generation, and of baby boomers.
Methods
This cross-sectional study used secondary data from the 2016 Korea Health Panel Study, which was conducted to investigate the factors associated with health expenditures and unmet healthcare needs of single-person households through hierarchical multiple regression analysis.
Results
The subjective health status of a single household showed a significant interaction with pre-baby boomers (β=.16, p=.045) in health expenditure. Identifying as men (OR=1.59, p=.046) and subjective health status (OR=1.90, p=.001) were statistically significant in terms of unmet healthcare needs. However, there was no significant interaction between pre-baby boomers and unmet healthcare needs.
Conclusion
Baby boomers are the first to be prepared for their later years in the current aging society. Despite a stable financial status due to vital economic activities, social support for baby boomers is inadequate. The rights guaranteed to family members under the system centered around kinship should also be guaranteed to single-person households.
This study aimed to compare the health expenditure and unmet health care needs and factors associated with these, in single-person households pre- and post-baby boomer generation, and of baby boomers.
This cross-sectional study used secondary data from the 2016 Korea Health Panel Study, which was conducted to investigate the factors associated with health expenditures and unmet healthcare needs of single-person households through hierarchical multiple regression analysis.
The subjective health status of a single household showed a significant interaction with pre-baby boomers (β=.16, p=.045) in health expenditure. Identifying as men (OR=1.59, p=.046) and subjective health status (OR=1.90, p=.001) were statistically significant in terms of unmet healthcare needs. However, there was no significant interaction between pre-baby boomers and unmet healthcare needs.
Baby boomers are the first to be prepared for their later years in the current aging society. Despite a stable financial status due to vital economic activities, social support for baby boomers is inadequate. The rights guaranteed to family members under the system centered around kinship should also be guaranteed to single-person households.
With industrialization, the family structure in South Korea evolved from traditional to nuclear and single-person households, where individuals live alone and earn a livelihood independently [1]. The number of single-person households in South Korea increased by 1,428% from 382,743 in 1980 to 6,643,000 in 2020, constituting 31.7% of the total number of households [2]. Concurrently, the life expectancy in Korea rapidly increased from 62.16 (men 58.70, women 65.80) in 1970 to 83.3 (men 80.3, women 86.3) in 2019, the second highest among the Organization for Economic Cooperation and Development (OECD) countries. Consequently, the share of the population aged 65 years and older increased from 3.1% in 1970 to 14.9% in 2019 [3]. In this scenario of aging population and falling birth rates, the number of single-person households will continue to increase. In particular, women single-person households, the numbers of which are approximately three times higher than those of men single-person households, are expected to become a common occurrence in coming years [4].
The reasons for the increase in the number of single-person households vary. Increasingly, more young adults show a preference to remaining unmarried because of changing views on marriage, and focus instead on studying or career advancement to develop competencies in a competitive society [5, 6]. Among middle-aged adults, living alone is usually the result of separation or divorce, while older adults find themselves alone after the death of their spouse and children moving out [1]. When a single-person household is exposed to disease or disability during this period, it is essential to provide care services.
The total government and compulsory spending on Long Term Care (LTC) for population aging accounted for 1.5% of Gross Domestic Product (GDP) across OECD countries in 2021 [7]. Korea (1.1% of the GDP) allocated less than the OECD average. Since the health insurance system was applied to all Koreans in 1989, the government and compulsory insurance spending on LTC (health) was for inpatient LTC, which accounted for 76% of all LTC spending [8]. Single-person households are more likely to experience the burden of health expenditures owing to high living expenses and weak financial conditions. Health expenditures can be a significant financial pressure at both the household and national levels, and deprive individuals of the right to healthcare in the absence of an increase in household income. In particular, single-person households among middle-aged or older adults have higher healthcare expenses [8]. Individuals born between 1955 and 1963, immediately after the Korean War, are defined as baby boomers. A portion of this generation will enter the later years of their lives by 2020.
Compared to other age groups, older adults have higher healthcare utilization and dependency owing to a higher morbidity rate of chronic diseases and reduced ability to perform everyday tasks [9], and the psychological and financial burden is especially high for single-person households. According to Jun [10], among the patterns of consumption expenditure of single-person households, health expenditure is attributed to old age, low educational, and income level. Specifically, health expenditures of single-person households can lead to a blind spot in healthcare and unmet healthcare needs.
Unmet healthcare needs are indices of the difficulties faced when using healthcare services [7]. In other words, they refer to a situation in which a person does not receive adequate healthcare services when required. Even though Korea achieved universal coverage through the mandatory National Health Insurance (NHI), the public sector accounts for about 60% of total health expenditure, well below the 71% of health care spending on average in OECD countries [7]. Similarly, unmet health care needs are a serious issue among older people in Europe, who experience various senile diseases, including functional decline and physical illness [11, 12], thereby requiring long-term care and more health care than other generations [13]. In the absence of unmet healthcare needs, diseases can be prevented, and suitable treatments can be provided. When treatments are not provided in a timely manner, it can lead to increased disease severity, possibility of complications, and higher death rates. Hence, unmet healthcare needs have a negative influence on overall health and quality of life [14].
Previous studies assume that the basic unit of monetary expenditure is the household and not the individual, given that each individual’s welfare is related to the income of all household members [15]. This assumption is problematic because it disregards the implications of the state of health of an individual in a single-person household with regard to patterns of personal expenditures, including those on healthcare [16].
The aging of baby boomers will increase health services and care needs. However, there is limited information on the next generation that will experience caregiving burden after the baby boomer generation [17, 18]. Therefore, this study aimed to compare the health expenditure and unmet health care needs and factors associated with these, in single-person households baby boomer generation.
This cross-sectional study was a secondary analysis of the dataset of the 2016 Korea Health Panel Study (version 1.5) conducted by the Korea Institute for Health and Social Affairs and the National Health Insurance Service.
This study analyzed the 2008~2016 data of the Korea Health Panel Survey (KHPS), a government approved statistical survey. Sampling was performed with a stratified method using 90% of the 2005 census data. From the 6,437 households identified in the data collected from 2008 to 2016, we selected 1,259 single-person households that reported unmet healthcare needs. A total of 1,256 households were finally selected after excluding two households with members under 20 years old (set as the lower limit based on this being the age when people generally become economically active) and one household in which the subject was an unpaid family worker. Unpaid family workers are family members or relatives of self-employed individuals who work for at least one-third of their regular working hours without being paid.
Health expenditure and unmet healthcare needs were set as dependent variables to analyze the status of medical services according to the generation of the single-person households. These variables were useful for evaluating medical access in healthcare systems. By considering these two variables simultaneously, it is possible to respond to the health accessibility problem accurately [19].
Health expenditures were measured using the Xu method proposed by the World Health Organization (WHO) and calculated based on the percentage of health spending over a household’s capacity to pay [20]. Health expenditures are defined as the sum of health and medical care, medicine, medical supplies, and medical equipment purchases. Health and medical care expenditures included emergency care, hospitalization, outpatient treatment, and costs related to transportation, inpatient care, postnatal care, and postnatal care workers. Inpatient care expenditures were obtained by multiplying the number of days of hospitalization with the number of hours of care. Medicine expenditures included emergency, inpatient, and outpatient prescriptions, general medications, traditional Korean medicine, and medicines taken for more than three months. Expenditures for medical supplies and equipment included general quasi-drugs, eyeglasses or contact lenses, as well as the costs for purchasing, leasing, and repairing medical equipment.
Unmet healthcare needs were evaluated from subjective (considering subjects’ opinions) and objective (the difference between the required and actual medical services) perspectives [21]. While objective unmet healthcare needs can be measured and thus generalized, subjective unmet healthcare needs are a more comprehensive representation of individual perspectives. Accordingly, this study conducted a comprehensive evaluation by considering both the perspectives. A response of "yes, more than once" to the question, "have you ever not been able to visit the hospital or clinic (not including a dental clinic) even though you wanted to visit it in the past year?", which was included in the 2016 Korea Health Panel Study, was considered representative of unmet health care needs.
In this study, sex, marital status, education level, subjective health status, chronic disease, and income were considered as factors influencing health expenditure, and unmet healthcare needs [19, 22]. In previous studies, unmet household health care needs did not show consistent results. Smoking and the use of medications, which are important variables, were added, whereas income was removed according to previous empirical analyses.
The baby boomer generation in South Korea is associated with fewer children and nuclear families due to a low birth rate [23]. The pre-baby boomer generation, characterized by low income, and the baby boomer generation can face the economic burden of healthcare costs from both the household and national perspective. The baby boomer generation (those born between 1955 and 1963 [23]) in South Korea is associated with fewer children and nuclear families due to a low birth rate [23]. In this study, age as a continuous variable was categorized as the pre-baby boomer generation for those born before 1955, and baby boomers for those born between 1955 and 1963.
Subjective health status is a self-reported indicator of psychological and physical health status [24]. Items were scored on a five-point Likert scale, where five points indicated poor health status and one point indicated excellent health status.
The KHPS uses 298 diagnostic codes that were developed based on the Korean Standard Classification of Diseases and modified national versions of the International Statistical Classification of Disease and Related Health Problems. Seven chronic diseases were included in this study: hypertension, diabetes, hyperlipidemia, arthropathy, tuberculosis, ischemic heart disease, and cerebrovascular disease, which were selected based on the associated high medical costs.
Data on single-person households were consolidated and analyzed based on the household serial numbers and identification numbers. The collected data were analyzed using SPSS 25.0. We calculated the frequency and percentage for each variable and evaluated the differences between the groups using the chi-square test and independent t-test. The factors associated with health expenditures and unmet healthcare needs were analyzed using a hierarchical multiple regression analysis and hierarchical logistic regression analysis. Hierarchical regression is used to verify whether the variables of interest explain a statistically significant amount of variance in the dependent variable after accounting for all the other variables. In addition, to compare the characteristics of the pre-baby and baby boom generations, an interaction variable that combines independent variables with the two generations was used to estimate the difference between them. We focused on whether Model 2 explained the health expenditures adjusting for sex, age, and marital status in Model 1 to reduce bias in estimating the effects on baby boomer generation.
The regression analysis helps to examine the R2 change and F-statistic change between the two models, in addition to reporting the level of significance for each model. We conducted a multicollinearity test because of possible correlations between the study variables. There was no indication of multicollinearity for any of the variables.
The Korea Health Panel Study was conducted after informed consent was obtained from all subjects. For this study, prior to its commencement, a data use agreement was submitted to obtain approval from the Korea Institute for Health and Social Affairs (Approval No. 2019-02).
The number of men and women subjects from the baby boomer generation was 152 (46.1%) and 178 (53.9%), and from the pre-baby boomer generation was 161 (17.4%) and 765 (82.6%), respectively. The number of women subjects was 4.75 times higher than that of men subjects. In terms of the educational level of the pre-baby boomers, 466 subjects (50.4%) were elementary school graduates and 205 (22.1%) had a lack of schooling. In contrast, in the baby boomer generation, 135 subjects (40.9%) were university graduates or higher and 115 (34.9%) were high school graduates, thus showing a higher level of education than the previous generation. For both men and women, subjective health status was higher in younger subjects. The two groups showed statistically significant differences in all characteristics except for the number of medications taken (Table 1).
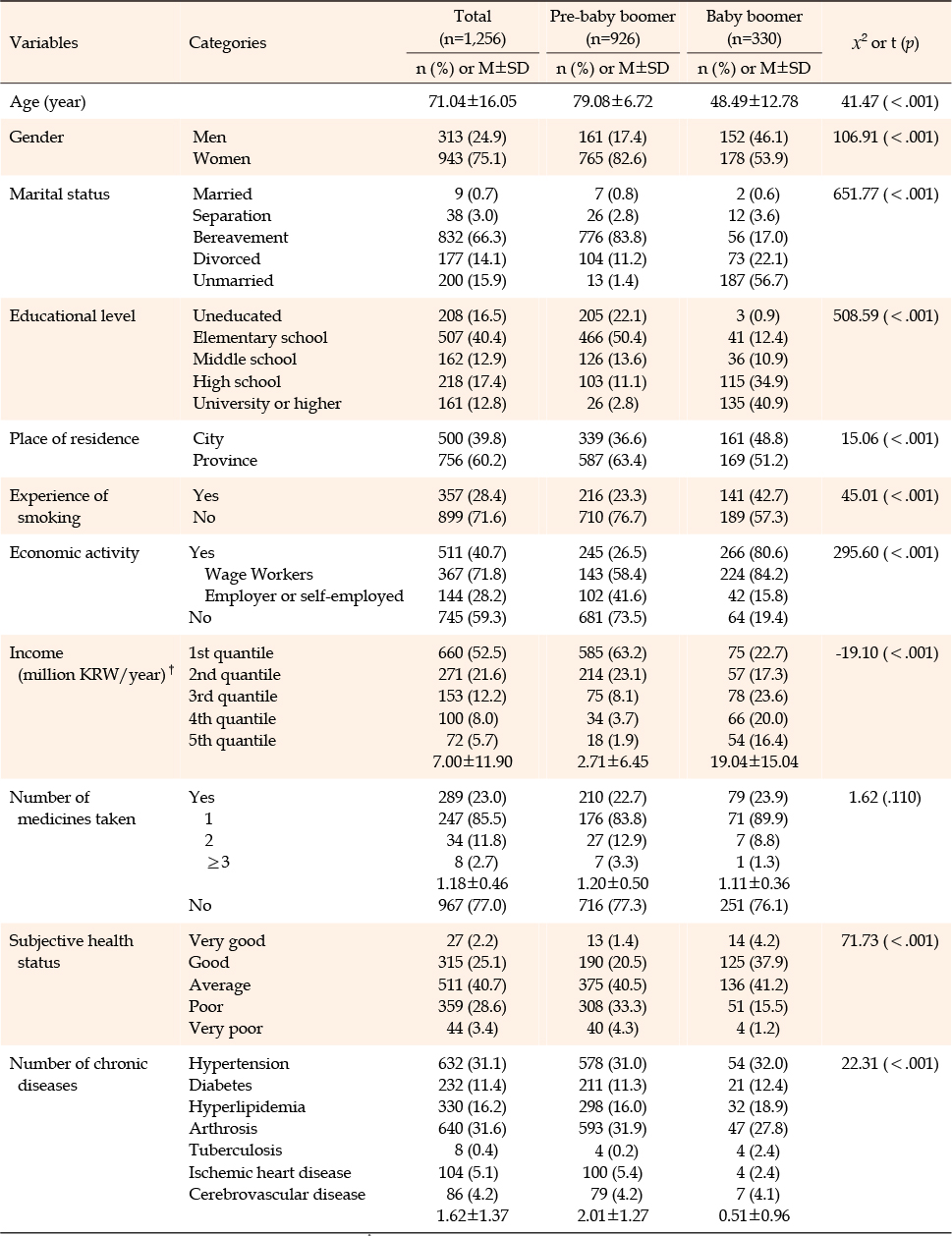
Table 1
Demographic Characteristics of Sample
The average annual health expenditure of single-person households was 1,179,600 Korean won. The average annual health expenditure of the pre-baby boomers was 1,315,700 Korean won while that of the baby boomer generation was 797,600 Korean won. Health expenditure was significantly higher in the pre-baby boomer generation than in the baby boomer generation (t=5.00, p<.001) (Table 2). Most of the health expenditure was related to medical services, wherein the expenditure of purchasing medications and medical supplies in the baby boomer generation comprised 21.8% of the total health expenditure (Figure 1-A).
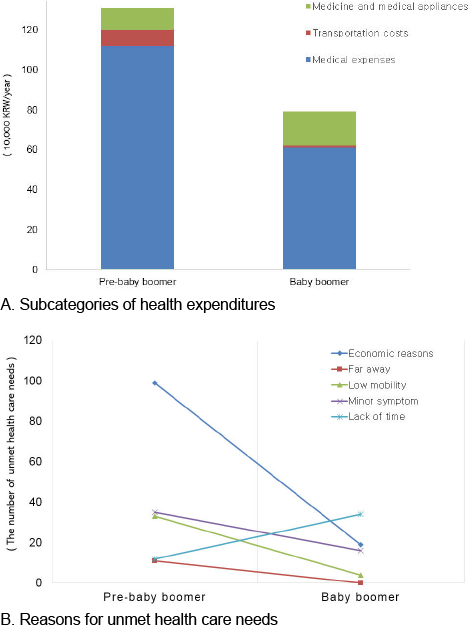
Figure 1
Subcategories of health expenditures.
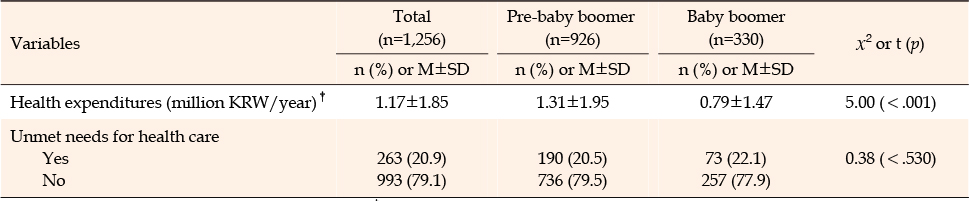
Table 2
Health Expenditures and Unmet Health Care Needs
The unmet healthcare needs of pre-baby boomers were 190 (20.5%), and 73 (22.1%) of baby boomers, but there was no statistically significant difference between generations (χ2=.38, p=.530) (Table 2). The most important reason for unmet health care needs was financial burden (52.1%) for the pre-baby boomers and a lack of time to visit medical institutions (46.6%) for the baby boomers (Figure 1-B).
A hierarchical multiple regression analysis was performed to identify the factors associated with health expenditure (Table 3). The Durbin-Watson statistic had a value of 2.00, and its proximity to 2 proved the independence of the residuals. As the variance inflation factors were less than 10, there was no issue with multicollinearity in these models. Single-person households reporting "unmarried", "good subjective health status", and "no chronic diseases" were more likely to increase health expenditures than those reporting "with spouse", "bad health status", and "chronic diseases" in Model 2 (β=.06, p=.033; β=.07, p<.001; β=.08, p=.001, respectively). The subjective health status of a single household showed a significant interaction among the pre-baby boomers (β=.16, p=.045), indicating that the subjective health status was affected by the generations. In other words, when the subjective health status of the pre-baby boomers worsened, their health expenditure was higher than that of the baby boomers.
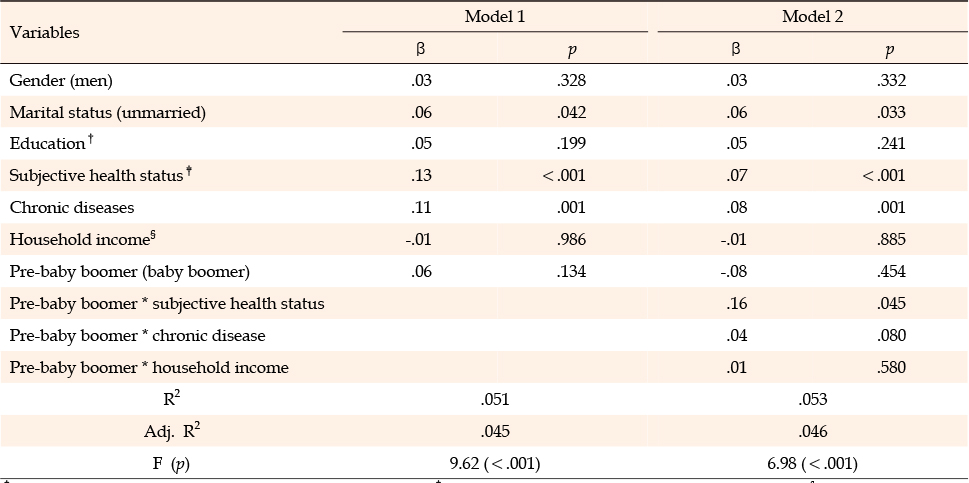
Table 3
Influencing Factors on the Health Expenditures in Single-Person Households
A hierarchical logistic regression analysis was performed to identify the factors associated with unmet healthcare needs. The regression model was statistically significant (Hosmer & Lemeshow, χ2=3.27, p=.859), with an explanatory power of 5.0%(Nagelkerke, R2=.05). Compared to people who reported being men and having better subjective health status, those reporting being men and having worse health status were significantly more likely to have unmet health care needs (OR=1.59, p=.046; OR=1.90, p=.001, respectively) after adjusting for demographic characteristics. There was no significant interaction between generations (Table 4).
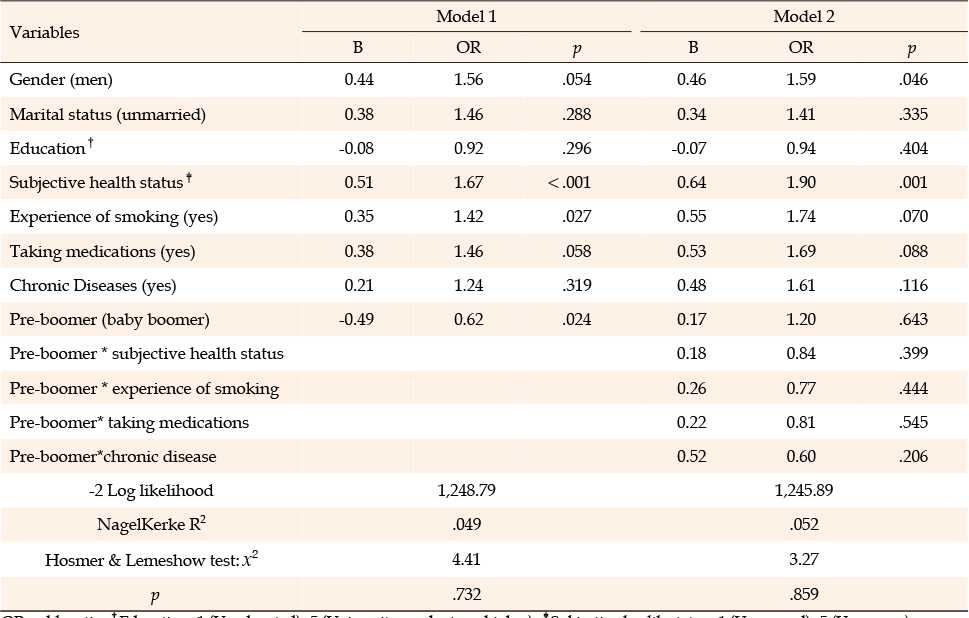
Table 4
Influencing Factors on the Unmet Health Care Needs in Single-Person Households
Globally, baby boomers have experienced explosive population and economic growth. Thus, this generation is believed to have a better health status than the previous generation [25]; however, health management is becoming increasingly important for baby boomers in their retirement years. In particular, single-person households experience a lack of family care and weakened financial status, in addition to the burden of health management, which may lead to health inequality. Hence, health expenditures and unmet healthcare needs were considered key factors in the health management of single-person households in this study.
It can be inferred that owing to their age, the subjective health status of the pre-baby boomer generation is "poor" or "very poor", thereby leading to higher medical demands. Moreover, health expenditures accounted for 48.5% of their annual income. In contrast, the annual average health expenditure of the baby boomer generation was lower than the total health expenditure of single-person households, yet this may have been a burden for individuals. Medical services are used at a personal level; however, such expenses can be shared within a household. The baby boomer generation, which is preparing for retirement, feels overburdened by health expenditures for personal health management owing to its unstable financial status when compared to the previous generation, which ultimately has a potential risk of having a negative effect on health. Furthermore, 56.7% of the single-person households in the baby boomer generation were unmarried. A previous study reported that unmarried people with low incomes are more likely to be overburdened by health expenditures [26] because of self-centered spending habits, irrational consumption expenditures, lack of interest in health, and inadequate preparation for the future [27]. When the subcategories of health expenditures were analyzed, it was found that 21.8% of health expenditures in the baby boomer generation were associated with medicines and medical supplies. This result is similar to the findings of a previous study on the trend of spending habits in single-person households in their 20s and 30s, in which spending on Korean medicine or nutritional supplements was higher than that in multi-person households [28]. Accordingly, further research is necessary since marital status is considered to influence health expenditures.
Approximately 21.0% of single-person households experienced unmet healthcare needs, regardless of age. This figure is higher than the 16.9% reported in a study on adults aged 65 years and above in 2015 [29] and 11.81% in a study on adults aged below 65 years in 2017 [30]. This indicates that using medical services is difficult in the absence of family members who can provide assistance, and there is no policy or possibility to call an emergency service. Another study reported that single-person households had a higher rate of experiencing unmet healthcare needs than married couples [30]. Hence, further research is needed to guarantee the right to health in single-person households.
In this study, the factors associated with health expenditure were age, marital status, subjective health status, and chronic diseases. It can be inferred that individuals become vulnerable to increasing health expenditure as they age. Previous studies have reported a similar relationship between age and health expenditures [26, 31]. In addition, individuals who lived alone but without a spouse had higher health expenditure than those with a legal spouse. Therefore, this result supports the findings of this study, in which single-person households had a higher burden of health expenditures. In previous studies, middle-aged or elderly women with low incomes had higher health expenditures than their men counterparts [26, 32, 33]; however, no statistically significant difference was observed among single-person households in this study. After adjusting for demographic characteristics, subjective health status and chronic diseases were found to be associated with health expenditure. As reported in previous studies [26, 33, 34], health expenditures were higher when the subjects had poor subjective health status. In line with a previous study conducted among older adults with low incomes [32], health expenditures increased if the subjects had a chronic disease. Regardless of household type, chronic diseases require lifelong care and management, thus increasing health expenditure.
The factors associated with unmet healthcare needs in single-person households were sex, pre-baby boomer group, and subjective health status. Men subjects experienced 1.59 times higher unmet health care needs than women subjects because they lacked sufficient time to visit medical institutions, mostly owing to their generally higher employment rate [35]. This result corresponds to the lack of time to visit a medical institution, which is generally known as the most significant reason for unmet healthcare needs in the baby boomer generation. In this study, subjects with poor subjective health status had higher unmet healthcare needs than those with good subjective health status owing to financial or time issues. There was no significant difference between generations in terms of unmet healthcare needs in single-person households. A previous study [36] showed that the level of unmet healthcare needs according to household type was highest in single-person households, lower in cases of cohabitation of a couple, and lowest in cohabitation with children. Moreover, elderly individuals who lived alone experience difficulties when visiting hospitals because of a lack of social support. A scoping review of the unmet care needs of older people suggested that unmet nursing care needs varied and were geographically widespread in terms of the physical, psychosocial, and spiritual needs [37].
Subjective health status is a crucial factor in health expenditure and unmet healthcare needs in single-person households. Baby boomers were the first to enter their later years in the current aging society. Care, and policy measures to support single-person households of this generation are urgently needed because of their weakened financial status, lack of social support, and vulnerability to poor health. A longitudinal cohort study of self-rated health has shown that there is no evidence that baby boomers are healthier as they age or less healthier than previous generations [38]. Therefore, interventions targeting the entire population are suggested as a way to improve subjective health status and reduce the need for healthcare and its related costs [38].
Our study has several limitations. As a cross-sectional study, the associations found in this analysis cannot be interpreted as influencing factors with specific causality. Moreover, this study only analyzed responses to survey questions; thus, factors that were not investigated in the survey questions could not be assessed. Second, because the two age groups (baby boomers and post-baby boomers) occupy different life cycle stages, age can affect other independent variables. In this study, the health expenditure, and unmet needs of single-person households in the baby boomer generation were identified; however, future studies on the physical health level and quality of life according to their economic level need to be conducted. Third, there were differences in general characteristics between the pre-baby boomer and baby boomer generations. However, in the KHPS data, single-person households of people born between 1955 and 1963, that is, the baby boomer generation, accounted for only 10% of the total single-person households, making it difficult to ensure homogeneity between generations. Therefore, future studies should include propensity score matching for a more detailed analysis.
Declining family sizes and an increase in single-person households are recent noticeable changes in the family structure of South Korea. A decrease in family size leads to the loss of family care and weakens household purchasing power, which ultimately reduces health expenditure, leading to potential health risks. In this study, the factors associated with the health expenditure of single-person households were being men, unmarried, and subjective health status, which showed a difference between the pre-baby and baby boomer generations. However, there was no difference between generations regarding unmet healthcare needs among single-person households. These findings suggest that special attention should be paid to ameliorate the subjective health status of single-person households. The health problems of single-person households in the baby boomer generation are critical, and health expenditures and unmet healthcare needs represent key indices of social welfare. The rights guaranteed to family members under the system centering around kinship, such as in Korean culture, should also be guaranteed fairly to single-person households. To ensure that healthcare resources are allocated for the benefit of the population, healthcare providers and the government should consider strategies to improve the equitable distribution of these resources.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - RD and RE.
Data collection - RD and RE.
Analysis and interpretation of the data - RD and RE.
Drafting and critical revision of the manuscript - RD and RE.
 E-SUBMISSION
E-SUBMISSION