
Purpose
Lung cancer (LC) is the leading cause of cancer-related death globally, and understanding symptom clusters (SCs) among LC patients could improve symptom management. This scoping review provides a comprehensive summary of the most common SCs and their compositions identified in studies specifically investigating SCs of LC patients.
Methods
A scoping review was conducted following the Joanna Briggs Institute methodology. The study included LC patients as participants, SCs as the concept, and studies with distinct aim to investigate LC SCs as the context. We searched studies from inception to September 2022 in PubMed, Embase, PsycINFO, CINAHL, and the Cochrane Library databases using the terms: "lung cancer," "cancer survivors, " and "symptom cluster." Results: Of 41 reviewed reports, 188 SCs were identified. Both a priori and de novo method were used to identify LC SCs, with exploratory factor analysis being the most commonly used statistical method in the de novo approach. The three most frequent SCs were respiratory, gastrointestinal (GI), and psychological SCs. The most common respiratory SC included cough + dyspnea. Nausea + vomiting was the most prevalent cluster membership among GI SCs. Sad + feeling irritable + feeling nervous + worrying was the most common cluster membership among psychological SCs.
Conclusion
Respiratory, GI, and psychological SCs were common among LC patients, and addressing these clusters could improve symptom management strategies. Further research on SCs across the lung cancer trajectory is essential to enhance our understanding about SCs and facilitate effective symptom management throughout the disease course.
Lung cancer (LC) is the leading cause of cancer-related death globally, and understanding symptom clusters (SCs) among LC patients could improve symptom management. This scoping review provides a comprehensive summary of the most common SCs and their compositions identified in studies specifically investigating SCs of LC patients.
A scoping review was conducted following the Joanna Briggs Institute methodology. The study included LC patients as participants, SCs as the concept, and studies with distinct aim to investigate LC SCs as the context. We searched studies from inception to September 2022 in PubMed, Embase, PsycINFO, CINAHL, and the Cochrane Library databases using the terms: "lung cancer," "cancer survivors, " and "symptom cluster."
Of 41 reviewed reports, 188 SCs were identified. Both a priori and de novo method were used to identify LC SCs, with exploratory factor analysis being the most commonly used statistical method in the de novo approach. The three most frequent SCs were respiratory, gastrointestinal (GI), and psychological SCs. The most common respiratory SC included cough + dyspnea. Nausea + vomiting was the most prevalent cluster membership among GI SCs. Sad + feeling irritable + feeling nervous + worrying was the most common cluster membership among psychological SCs.
Respiratory, GI, and psychological SCs were common among LC patients, and addressing these clusters could improve symptom management strategies. Further research on SCs across the lung cancer trajectory is essential to enhance our understanding about SCs and facilitate effective symptom management throughout the disease course.
Globally, lung cancer is the leading cause of cancer-related death, accounting for an estimated 2 million cases and 1.8 million deaths reported in 2011 [1]. Lung cancer patients often experience a high symptom burden, both emotional and physical, due to the disease itself and treatments such as chemotherapy [2], or surgery [3]. These symptoms significantly impact their quality of life [4]. Commonly reported symptoms among lung cancer patients include cough (87%), breathlessness (61%), and chest pain (58%) [5]. Additionally, fatigue and weight loss are frequently seen in those with advanced stages of the disease [6]. Given the complex and diverse nature of these symptoms, it is crucial to investigate the symptom experiences of lung cancer patients to enhance symptom management and overall patient care.
Symptom Clusters (SCs) are groups of two or more related symptoms that occur together and may or may not share same etiology [7]. These symptoms are not random groupings of symptoms but are usually interconnected, and their interaction can lead to a compounded effect on patient outcomes [8, 9]. The symptoms within a cluster interact and have a progressively strong effect on patient outcomes compared to individual symptoms; thus, SCs are crucial for clinical practice [10]. Effective symptom management can be achieved by considering SCs to better understand the patients’ symptom experience.
A comprehensive review of reports on SCs among lung cancer patients could enhance our understanding of lung cancer-related SCs and symptom management strategies. Although previous reviews have explored SCs in this patient group, their scope has been limited. A narrative literature review of SCs among lung cancer patients included only five reports [11]. In contrast, a recent scoping review on the SCs of lung cancer patients encompassed 53 articles covering 48 studies. However, this review employed a broad definition of SC, including reports that measured multiple co-occurring symptoms, regardless of whether the study’s primary aim was to investigate symptom clusters. This approach may have limited the depth of the findings [12]. Symptoms were grouped into a limited number of broader symptom categories, encompassing a wide range of different symptom expressions. While this approach provides a comprehensive overview, narrowing down symptoms into broader but limited number of symptom categories did not sufficiently differentiate each symptom, thus not adequately reflecting their unique characteristics in SC analysis. So far, no scoping review has summarized common SCs and, the specific symptom memberships by reviewing studies with distinct aim to investigate SCs. Additionally, there has no detailed examination of the analytic methods used to identify SCs in lung cancer patients.
The current scoping review aimed to provide a comprehensive understanding of SCs among lung cancer patients by exploring the methods used to identify SCs, the most common SCs, and their compositions in studies specifically focused on SCs.
The design of the study was a scoping review, which was performed in accordance with the Joanna Briggs Institute (JBI) methodology [13].
1) How are SCs identified among lung cancer patients in the studies which had distinct aim to investigate SCs? 2) What common SCs exist in lung cancer patients in the studies which had distinct aim to investigate SCs? 3) What are the compositions of common SCs identified among lung cancer patients in the studies which had distinct aim to investigate SCs?
The inclusion criteria were as follows: (i) participants were adults diagnosed with lung cancer at any stage, (ii) concept was SCs of lung cancer patients, and (iii) context as original reports with any type of design with distinct aim to investigate LC SCs. There were no restrictions regarding the type or phase of treatment, the time points for assessment, or the type of symptom assessments used, whether symptoms were measured by severity, occurrence, or distress. All types of study designs were included in this scoping review, except for review articles because the sources of the reviews had already been identified either through the database searches or from the manual search of the reference lists of the included reports.
The PubMed, Embase, PsycINFO, CINAHL, and Cochrane Library databases were searched from inception to September 2022. The search strategies were developed with the assistance of a librarian and included terms such as "lung cancer", "symptom cluster", and "cancer survivor" (Supplementary Table 1). The search was limited to reports published in English. Initially, 1138 reports were identified. The search was mostly updated on 31 November 2023, at which point the total number of reports reached 1743. These reports were then exported to EndNote X20, where duplicates were removed.
To select eligible reports, two authors (AJ and CYY) independently screened the titles and abstracts of all reports retrieved from the databases. They compared their screened results and selected reports by consulting a third reviewer. From the databases, a total of 1,743 reports were identified and screened based on their titles and abstracts, resulting in 60 articles being chosen for full-text screening. After applying eligibility criteria-such as the absence of a symptom cluster description, review paper, report paper, studies on other cancers, or papers in languages other than English-26 reports were excluded. Consequently, 34 reports were initially selected for the current study. A manual search of the reference lists in the selected reports identified 7 additional reports for inclusion. Ultimately, 41 reports were included in this review, as detailed in a PRISMA-ScR flow diagram [14] (Figure 1).
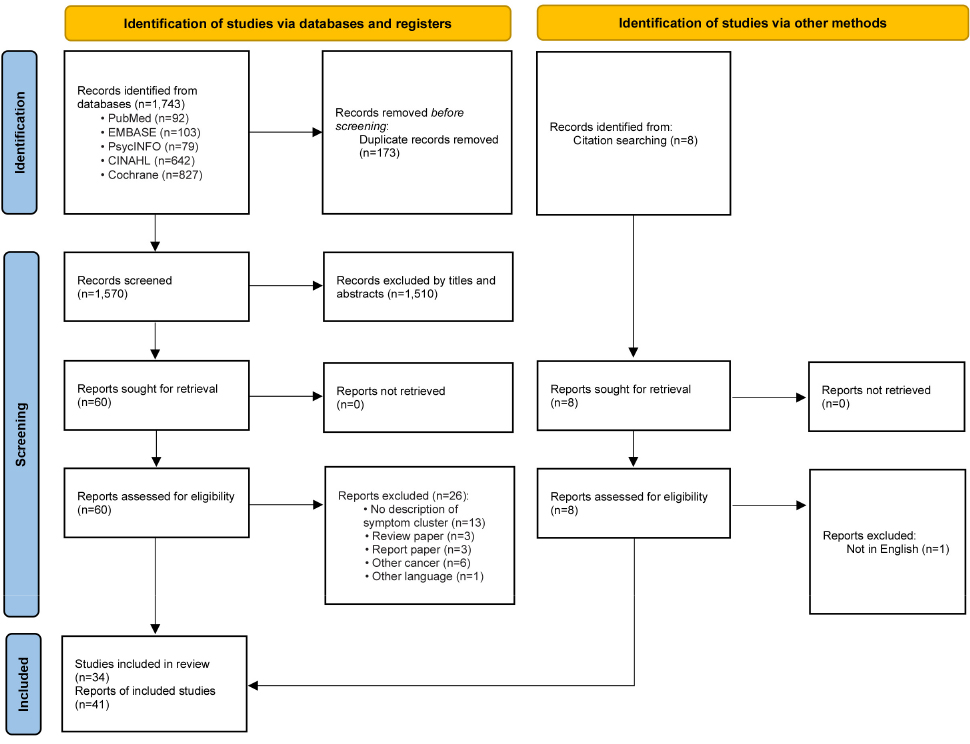
Figure 1
PRISMA flow diagram for report selection.
Two authors (AJ and CYY) independently extracted the following data by using the data extraction instrument suggested by the JBI scoping review methodology: study setting, study design, sample size, instrument used for symptom assessment, analytic technique used to identify SCs, the identified SCs, and symptom membership in each SC.
Some reports presented SC results from the same study (report ID #3 [A3] and 4 [A4], report ID #6 [A6] and 7 [A7], report ID #15 [A15] and 16 [A16], report ID #31 [A31] and 38 [A38]). Identical SC results obtained from the same study, using the same data and analysis methodology, were considered duplicates and thus treated as a single result from a single study with separate reports in the current review (report ID #3 [A3] and 4 [A4]). In the cases where reports employed different analytic techniques on the same study data and achieved different SC results, each result was considered as a separate result derived from a single study (report ID #6 [A6] and 7 [A7]). Distinct results from the same study data with different analyses, based on different compositions of symptom items, were considered separate results i.e. separate reports within a single study (report ID #15 [A15] and 16 [A16]). For results based on the same study data and the same analysis but utilizing different dimensions of symptoms, such as severity or occurrence, and achieving different results, each result was counted separately (report ID #31 [A31] and 38 [A38]). For SCs identified from longitudinal data ('report ID #2 [A2], 4 [A4], 5 [A5], 6 [A6], 7 [A7], 12 [A12], 16 [A16], 17 [A17], 20 [A20], 21 [A21], 24 [A24], 31 [A31], and 36 [A36]), the results from each time point were considered separately. For the reports identifying multiple results by analyzing multiple symptom dimensions or collecting data at multiple time points, an α bet letter was added to the report ID # to distinguish the SC result of each dimension or time point (e.g., report ID #5a, 5b, 5c, 5d; report ID #18a, 18b; report ID #20a, 20b, 20c, 20d, 20e, 20f, report ID #21a, 21b, 21c, 24a, 24b; report ID #31a, 31b, 31c, 31d, 31e, 31f; report ID #38a, 38b, which analyzed SCs based on symptom occurrence and severity at different time points using longitudinal data).
In accordance with the JBI methodology [13], the data about the lung cancer patients (participants) and symptom cluster (concept) were extracted. The general characteristics of the reports, such as study design and sample size, along with specific information about the lung cancer patient, including treatment received, were detailed. The instruments to measure symptoms, the methodologies employed to identify SCs, and the identified SCs were summarized and categorized. Symptoms that were measured based on symptom occurrence, severity, or distress and identified as SCs were organized accordingly. For identified SCs labeled as "no name," cluster membership was reviewed and categorized into a specific SC if more than half of the symptoms belonged to that SC. The SCs were listed, and frequently reported common SCs were identified. To clarify SC membership, specific cluster memberships of common symptom SCs are summarized in the tables.
A total of 10,829 participants were included, with individual reports ranging from 10 to 2,405 patients. Approximately 55% of the participants were male. The mean age of the participants ranged from 52 to 72 years. The study employed various designs, including cross-sectional, longitudinal, interventional and qualitative approaches. Nearly half of the reports applied a cross-sectional design (49%) [A1,A8-11,A13-15,A18,A22,A23,A28-30,A32-35,A38,A41]; and 32% adopted a longitudinal design [A2,A4-7,A12,A16,A17,A20,A21,A24,A31,A36]. Chemotherapy was the most frequently reported treatment modality for lung cancer, cited in 32% of the studies [A8,A9,A14,A17-19,A21,A23,A24,A31,A35,A38,A41]. Additionally, approximately 7% of the patients underwent radiotherapy [A2-4]. The earliest report of SCs among lung cancer patients was published in 1997. The reports were conducted in eleven countries: the U.S., the U.K., China, Thailand, Hong Kong, Sweden, Korea, Taiwan, Brazil, Japan, and Vietnam. Notably, 27% of the reports were conducted in the United States [A1,A6,A7,A9,A10,A12,A13,A30-32,A38] (Table 1).
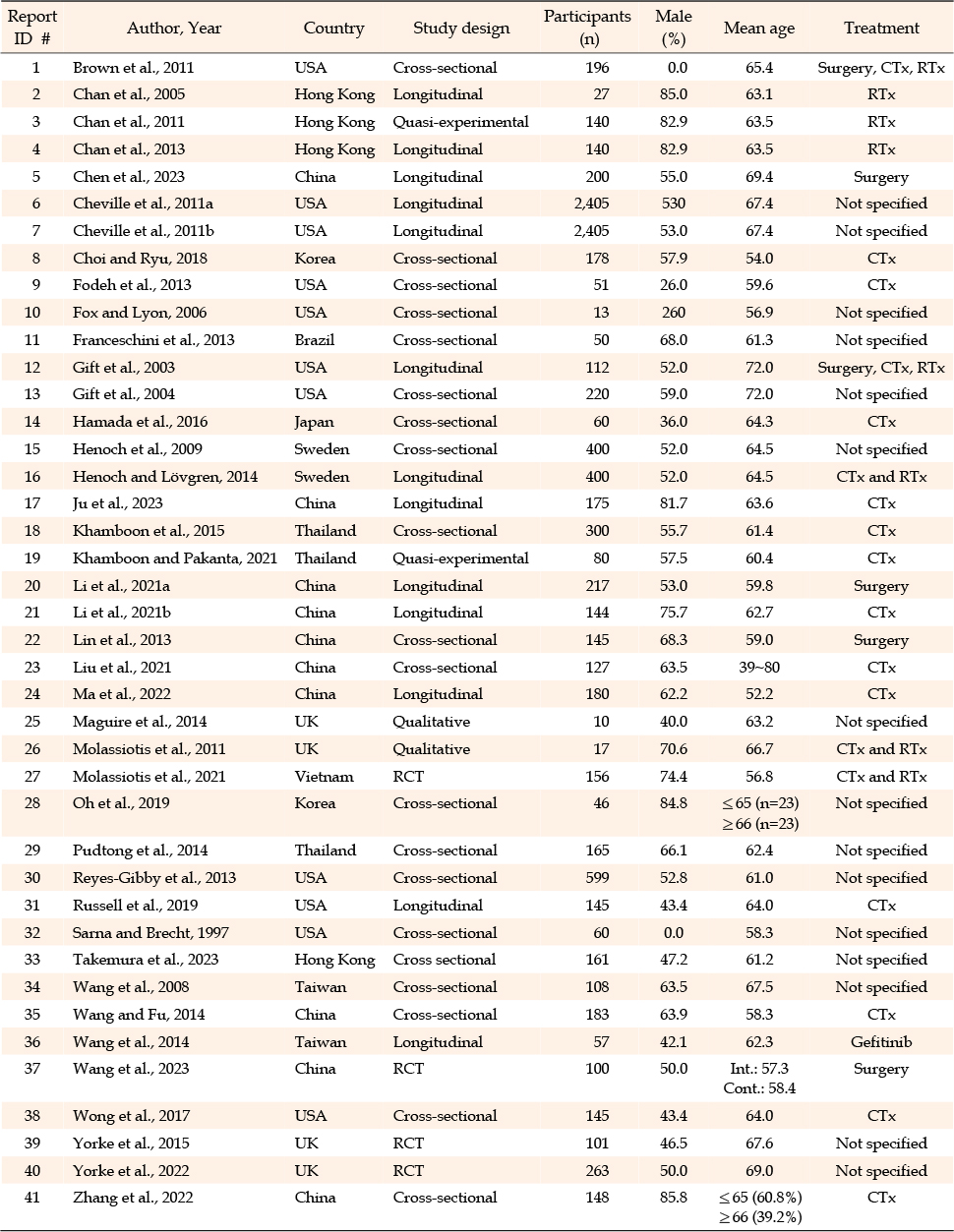
Table 1
General Characteristics of the Included Reports (N=41)
The measurement instruments used for symptoms and results are summarized in Supplementary Table 2. A total of 13 reports (32%) used the M.D. Anderson Symptoms Inventory (MDASI) [15], which was developed for a brief measure of the severity and impact of cancer-related symptoms [A5,A8,A14,A17,A20-A22,A24,A28,A34-A36,A41]. Four reports (10%) employed the Memorial Symptom Assessment Scale (MSAS) [A18,A29,A31,A38], and another four reports (10%) used European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) [A11,A15,A16,A23]. Three reports (7%) applied the Lung Cancer Symptoms Scale (LCSS) [A1,A6,A7], and another three (7%) used the Symptom Distress Scale (SDS) [A9,A15,A32]. An additional three reports (7%) utilized the Visual Analogue Scale (VAS) [A2-4]. Two reports employed the Numeric Rating Scale (NRS) [A37,A39], and two used the Physical Symptom Experience Tool (PSET) [A12,A13]. Reports also mentioned the use of the Short-Form 36 Health Status Survey (SF-36) [A10], Short-From 12 Health Status Survey (SF-12) [A30], ESAS [A19], and FACT [A27]. Symptoms were measured across two different dimensions in four reports where participants were receiving chemotherapy. Dimensions such as symptom occurrence and severity [A20,A31,A38] or symptom distress and severity [A18] were assessed using either the either MDASI-LC or MSAS. Commonly measured symptoms were identified among the various measurements used.
There are reports of the same instruments being used with different variations. To identify commonly measured symptoms, measurement instruments were categorized into 11 instruments that were specific to lung cancer symptoms.
SCs identified by occurrence and severity dimension shared congruent names and corresponding numerical patterns, whereas the actual composition of symptom membership diverged [A20,A31,A38]. This study identified five symptom clusters based on symptom distress or severity. Among these, two SCs shared identical names with similar composition of symptom memberships, while the remaining three were distinct SCs [A18].
A total of 17 reports identified SCs assessed them at multiple time points, ranging from three to seven [A2-7,A12,A16,A17,A20,A21,A24,A26,A27,A31,A36,A37] (Supplementary Table 2). Most of the designated time points were related to treatment, i.e., chemotherapy [A17,A21,A24,A31,A36], radiation therapy [A2,A3,A4], either chemotherapy or radiation therapy [A26,A27], surgery [A5,A20,A37], or any form of treatment [A16]. Three reports assessed symptoms at time points related to cancer diagnosis [A6,A7,A12]. Following baseline data collection, symptoms assessments were subsequently conducted from 6 days to 5 years.
SCs were identified through either an a priori method, where predefined SC membership was applied based on empirical evidence, or a de novo method applying a quantitative statistical analysis technique [16]. Two reports used a qualitative analytical approach [A25,A26]. Over half of the reports (56%) employed a de novo approach to identify SCs.
A priori analysis was used in 16 reports (39%) [A1-A4,A7,A9,A12,A16,A19,A22,A27,A30,A36,A37,A39,A40]. Gift et al. (2003) initially employed a priori analysis to identify a SC and evaluated the SC’s internal consistency with Cronbach's α. Most of the reports that adopted an a priori approach were published between 2003 and 2015 [A1-4,A7,A9,A12,A16,A22,A30,A36,A39], except for those that were part of intervention studies [A19,A27,A37,A40].
Among the de novo approach reports, Explanatory Factor Analysis (EFA) was the most commonly used statistical method (n=11) [A5,A6,A8,A14,A20,A21,A24,A31,A35,A38,A41]. Only a few reports specified the rotation method used: varimax [A6,A8,A35], promax [A14], orthogonal [A20], geomin [A31], oblique [A38], and maximal variation rotation [A41]. Principal Component Analysis (PCA) with varimax rotation was the second most frequently employed analytic technique for SC analysis (n=4) [A15,A18,A29,A32]. Two reports applied correlational analysis [A10,A33], and another two reports applied both factor analysis and hierarchical cluster analysis to identify SCs [A23,A34]. Studies employed the de novo approach were published between 2003 and 2023. There was a single report employing Latent Class Growth Analysis (LCGA) published in 2023, which aimed to explore longitudinal trajectories to identify subgroups of symptom clusters [A17].
A total of 188 SCs were identified in lung cancer patients. Among the SC studies with a priori approach, the respiratory SC was the primary focus of investigation. Dyspnea and cough were the main component of two SC memberships [A9,A16], while three SC memberships with fatigue [A1,A7,A39,A40], and four SC memberships addressed fatigue and pain [A37]. Dyspnea was also associated with fatigue and anxiety [A2-4,A26].
Overall, the three most common SCs identified among lung cancer patients, regardless of the analytic approach, were respiratory SCs (21%), gastrointestinal (GI) SCs (22%), and psychological SCs (14%). The remaining categories, no-name (12%) and other SCs (31%), are presented in Supplementary Table 3 and 4. In the SC studies with a de novo approach (n=164), one of the most frequently identified SCs was related to respiratory SC named as lung cancer-specific SC (n=18) and respiratory SC (n=15). Additionally, there were studies without specific names but associated with the respiratory SC because of the membership (n=3). GI SCs were identified almost as frequently as respiratory SCs, with categories including gastrointestinal SC, referred to as nutritional SC (n=15), gastrointestinal SC (n=14), digestive SC (n=3), anorexia SC (n=3), and SCs with no name (n=2). Overall, both GI SCs and respiratory SCs accounted for over 20% of the reports using the de novo approach. Psychological SCs were identified 25 times with the de novo approach and included names such as psychological SC (n=18), mental SC (n=4), emotional SC (n=4). One SC named "pain" and another with no name were categorized as psychological SCs considering their memberships.
A total of 39% of the reports included in the review identified respiratory SCs (40 times in 23 types), which were originally referred to as respiratory/respiratory function/respiratory distress/respiratory tract/pulmonary/lung cancer-related/lung cancer-specific SCs. The number of symptoms per cluster ranged from 2 to 8 symptoms (Table 2). Considering that dyspnea corresponds with breathing symptoms, shortness of breath (SOB) or difficulty breathing, three different cases of dyspnea were considered "dyspnea" for this review. For example, one report reported cough + difficulty breathing + shortness of breath as a SC [A31]; these findings were considered cough + dyspnea. Cough + dyspnea was identified as a single cluster 3 times (report ID #9 [A9], 15 [A15], 16 [A16]), and it was accompanied by fatigue (report ID #6 [A6], 7 [A7], 26 [A26], 39 [A39], 40 [A40]), expectoration (report ID #5a [A5], 21b [A21], 24a, 24b [A24]), chest tightness (report ID#31b [A31], 38a [A38]), or insomnia (report ID #18a [A18], 32 [A32]). Additionally, cough + dyspnea also clustered with chest tightness + expectoration (report ID #17 [A17], 20a [A20], 21c [A21]) and chest tightness + expectoration + pain (report ID #5b, 5c, 5d [A5]) (Table 2).
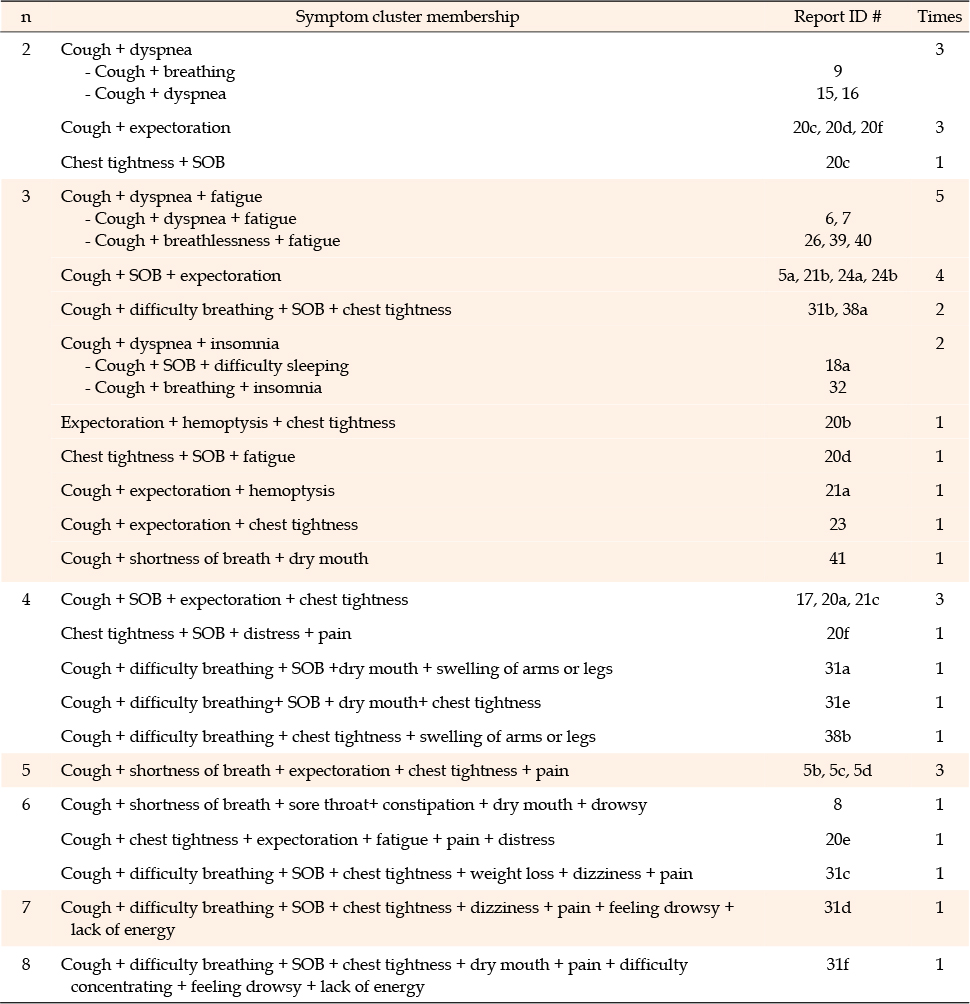
Table 2
Respiratory Symptom Clusters
GI SCs were identified in 37% of the reports (41 times, across 26 types) and were initially categorized under various names including nutritional, digestive function, digestive impairment, anorexia-related, fatigue-anorexia, epithelial-GI, treatment-related GI and other, GI distress, and GI SCs. These SCs consisted of 2 to 13 symptoms (Table 3). Nausea + vomiting was the most frequently identified SC (report ID #20b, 20e [A20], 21b, 21c [A21], 34 [A34], 35 [A35], 36 [A36], 41 [A41]. This cluster, Nausea + vomiting, also appeared in combination with constipation + lack of appetite (report ID #24a, 24b [A24]) and with lack of appetite + weight loss + fatigue + altered sense of taste + weakness (report ID #12a, 12b, 12c [A12], 13 [A13]). Additionally, nausea + vomiting also clustered with hair loss (report ID #18a [A18]), dizziness (report ID #18b [A18], numbness and dry mouth (report ID #28 [A28]), and appetite loss/anorexia + hypodipsia (report ID #23 [A23]). A unique cluster featuring of lack of appetite + increasing appetite + weight gain was identified in one report (report ID #31a, 31c [A31]), while lack of appetite + increasing appetite+ weight gain + weight loss was identified in two reports (report ID #31b, 31e [A31], 38a, 38b [A38]) (Table 3).
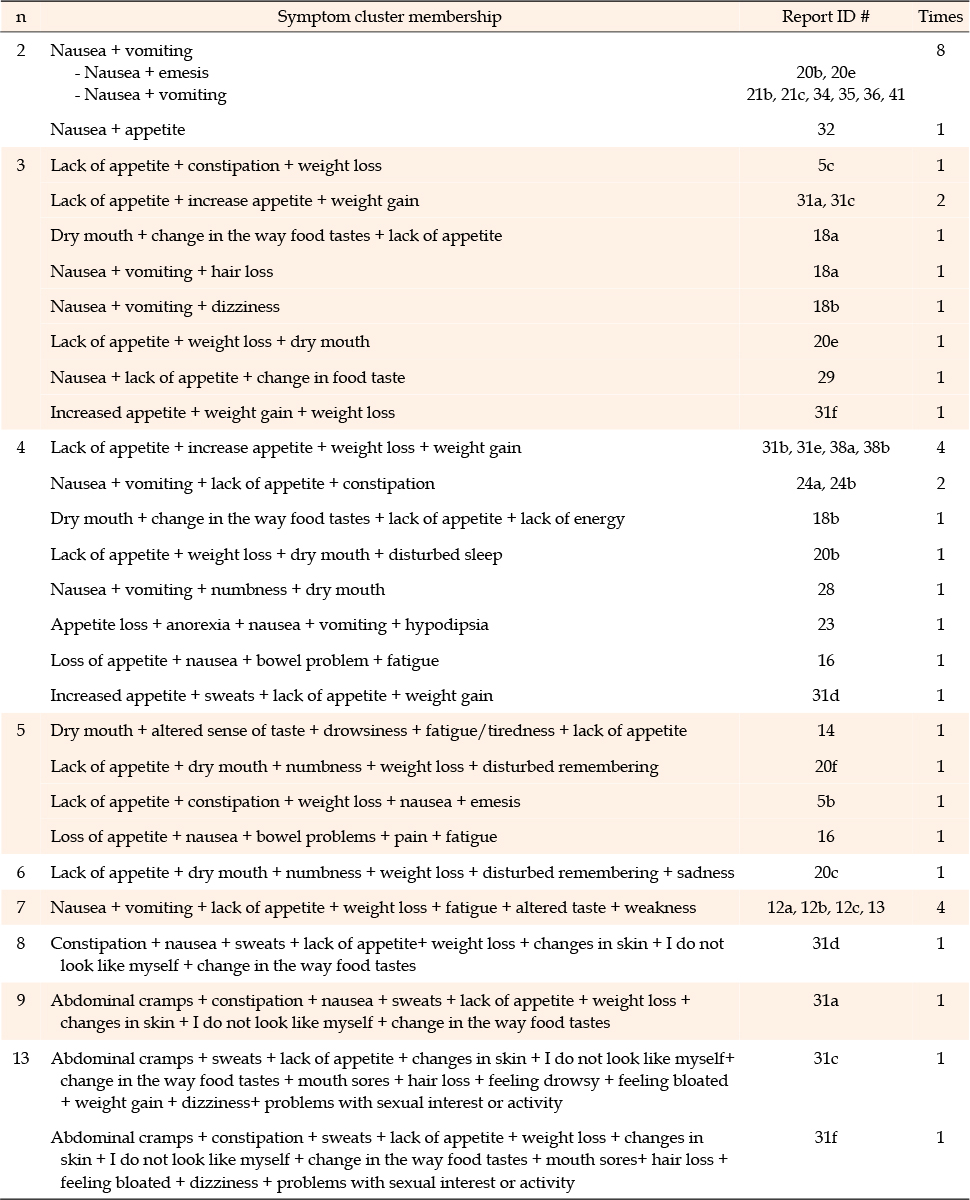
Table 3
Gastrointestinal Symptom Clusters
A total of 27% of the reports identified psychological SCs (26 times, 20 types), which were initially named psychological, psychological-somatic, global mental function, special mental function, mood, and emotional SCs. The "pain cluster" mentioned in the report ID #14 [A14] refers to a SC consisting of anxiety, sadness, and pain, and is thus classified as a psychological SC. The number of symptoms per cluster varied from 2 to 8 (Table 4). Sad + distress formed two membership SCs (report ID #24a [A24], 35 [A35]). Additionally, sad + distress were also clustered with memory disturbance in report ID #5a, 5b, 5c, 5d [A5]. Four symptoms-sad + feeling irritable + feeling nervous + worrying-were identified a total of 7 times across two reports. These symptoms were observed twice as a single cluster in report ID #31e [A31], and 38b [A38], and additionally, five more times in combination with other symptoms in report ID #31a, 31b, 31c, 31d [A31], and 38a [A38] (Table 4).
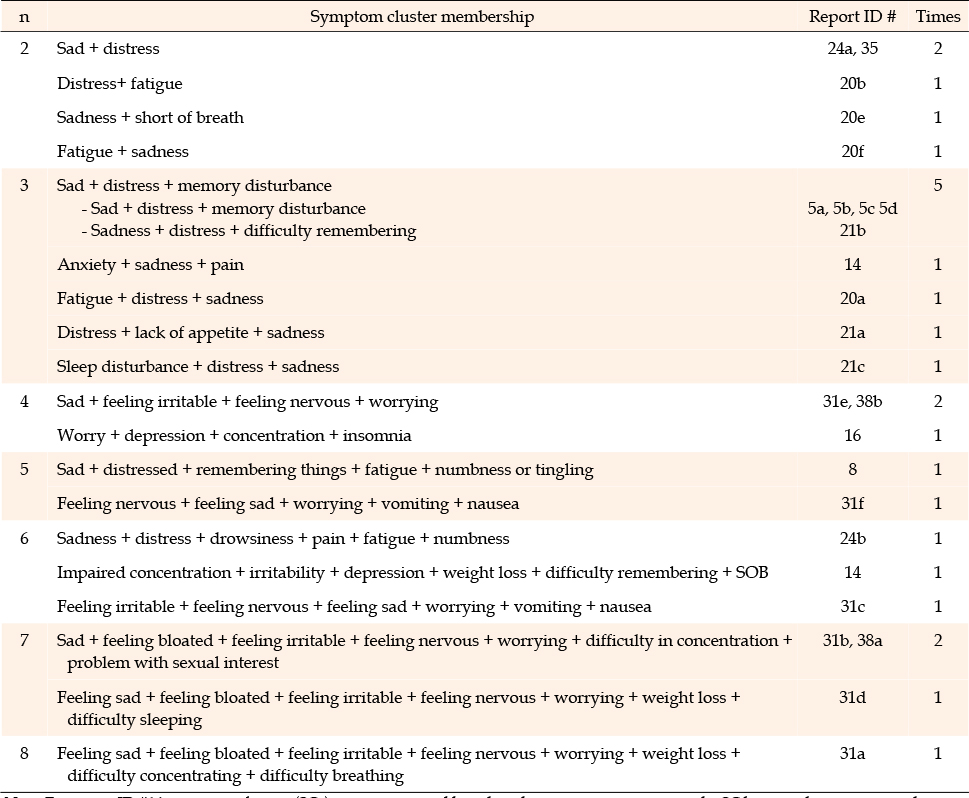
Table 4
Psychological Symptom Clusters
This scoping review provided a comprehensive overview of symptom clusters that were identified in studies of lung cancer patients. The three common symptom clusters among lung cancer patients were identified as respiratory SCs, GI SCs, and psychological SCs.
Various instruments were utilized to measure symptoms in the reports, with several symptoms commonly measured across them. There were two different conceptual approaches to symptom cluster research: a priori and de novo. In the current review, reports adopting the a priori approach were published earlier, between 2003 and 2015. Since then, there has been a shift toward the de novo approach, which employs statistical analysis techniques. Reports using the de novo approach have been published up to 2023, with the most recent report employing LCGA to identify subgroups of symptoms and longitudinal trajectories among homogenous patients, reflecting the lasted research trends.
The current review is consistent with the previous review, indicating that the majority of reports examining symptom clusters de novo, and there are statistical analytic methods such as factor analysis and cluster analysis in order to determine the number of symptom clusters and their symptom memberships [16]. Dong et al. (2014) reported relatively consistent results using PCA and HCA [17], although outcomes differed when using EFA. Two reports with de novo approach included in the current review applied multiple analytic techniques to identify lung cancer symptom clusters (LC SCs.) The findings from different analytic techniques, namely cluster analysis and HCA, and factor analysis combined with HCA, yielded consistent results. Approximately one-third of the studies employed longitudinal design. Regarding the stability of SC findings, the current study’s results partially align with those of the Dong et al., which supported instability, and partially with the findings of Rha et al. in 2019 and 2020, both of which suggested a relative stability of SCs. This includes recent studies reporting on stability of SCs [18, 19].
Another analytic approach to SC research is the identification of subgroups of patients who experience various levels of symptom burden within specific SCs. This method has been highlighted in prior studies, and one report in our review used latent class analysis [20]. The current review sheds light on the conceptual approaches employed in symptom cluster reports and emphasizes the need for further research to identify subgroups of patients who are vulnerable to higher symptom burden and poorer outcome [16].
Cough + dyspnea was the most frequently identified respiratory cluster membership. The finding aligns with the results of a previous narrative review of SCs among lung cancer patients [11]. Cough + dyspnea was identified as single cluster, and also clustered with fatigue. The current study results are consistent with the previous scoping review that fatigue is a frequently reported symptom throughout the entire course of the lung cancer [11]. This finding underscores the importance of early screening of cancer-related fatigue, as it significantly impacts patients’ quality of life [21]. The current review also identified that cough + dyspnea was associated with other co-occurring respiratory or related symptoms, such as expectoration, chest tightness, difficulty sleeping, chest tightness + expectoration, and pain + expectoration + chest tightness. These complex symptom interactions highlight the need for a comprehensive approach to symptom management, as respiratory symptoms often exacerbate other physical and emotional burdens [22].
It is understood that cough + dyspnea could be considered a common SC among those with respiratory SC, which could include additional respiratory or related symptoms. The close relationships between respiratory symptoms and other conditions such as fatigue, insomnia, or pain well depict complex symptom issues among lung cancer patients.
Nausea + vomiting was the most frequently identified GI SC. These findings are consistent with previous reviews of symptom clusters [17, 23, 24]. Similarly, this result corresponds to a previous review of symptom clusters in head and neck cancer in which approximately half of the studies identified nausea + vomiting as GI cluster memberships [25]. Although the participants in this review were receiving various treatments, the majority were undergoing chemotherapy, which is widely known to induce nausea and vomiting [26]. This may explain why these symptoms were frequently identified as part of the SCs. Consequently, future studies should consider investigating SCs based on different treatment modalities to better understand variations among patient groups. Additionally, this review also identified additional GI symptoms that could occur with nausea and vomiting, including lack of appetite and constipation, appetite loss/anorexia + hypodipsia, as well as non-GI symptoms such as hair loss, dizziness, numbness and dry mouth. Variations in patient characteristics, treatment types, symptom measurement, and the analysis method of symptoms may have contributed to the heterogeneity in the findings.
The third common cluster identified was a psychological SC. The predominant symptoms in the psychological SC were sad + distress. These findings are consistent with previous findings on SCs among head and neck cancer patients, in which approximately 38% of the reports identified sadness + distress as a psychological cluster membership [25]. Notably, sad + distress also clustered with other symptoms, and three clusters associated with memory disturbance were identified four times. The four symptoms, i.e., sad + feeling irritable + feeling nervous+ worrying, were identified as a single cluster, and these findings correspond with those of other studies of SCs in patients receiving chemotherapy [27]. Another systematic review of SCs among breast cancer patients reported that psychological SCs were similar but differed because they included anxiety and depression in addition to sadness, irritability, nervousness and worry [28]. Considering the repeated clustering of sad + feeling irritable + feeling nervous+ worrying in psychological SCs, it is essential to comprehensively assess psychological symptoms in lung cancer patients.
This review comprehensively identified common SCs and their memberships in lung cancer patients, which provides foundational information to nursing practice and research. Understanding common SCs and their membership can facilitate approaches to symptom management. Future studies should develop and evaluate interventions for symptom management that focus on the most frequently identified SCs and their memberships, such as cough + dyspnea, nausea + vomiting, and sad + distress. The association between respiratory symptoms and fatigue, insomnia, or pain indicates a need to investigate the underlying mechanisms shared by the symptoms involved in these SCs.
This review has some limitations. This scoping review included reports from 11 countries without restrictions on the countries included, limiting the reports to those published in English may have resulted in the omission of some relevant studies. Contradictory symptoms such as weight gain and weight loss, or lack of appetite and increasing appetite were reported in the same SCs based on the findings of the reports, which logically cannot occur simultaneously. This may indicate a measurement issue that could lead to misinterpretation of concurrent symptom experiences. Caution is needed when interpreting these results. There are only a few studies that have verified the association between influencing factors or the causal relationship of influencing factors to SCs, which require further investigation. Through this study, various analysis methods used to identify lung cancer-related symptom clusters were analyzed, and the results were summarized and presented. However, suggesting the most appropriate method for symptom cluster analysis was beyond the scope given the nature of a scoping review. The limited number of existing longitudinal studies with various treatments and time points restricted our understanding of changes in SCs. Although this scoping review has provided a comprehensive summary of current knowledge, future studies could leverage big data analyses from healthcare records to gain deeper insights into symptom cluster dynamics and influencing factors in larger, more diverse lung cancer populations. Longitudinal exploration of SCs will help understand the progression of SCs across the cancer trajectory.
This scoping review summarized SCs among patients with lung cancer. The most frequently observed SCs were respiratory, GI and psychological. Cough + dyspnea, nausea+ vomiting, and sadness + feeling irritable + feeling nervous + worrying were representative symptoms of common SCs. These SCs among lung cancer patients should be specifically addressed in oncology nursing practice. Further studies on SCs throughout the lung cancer trajectory could enhance understanding of SCs and improve symptom across the course of the disease.
Search TermsSupplementary Table 1
Results of Symptom Cluster Reports (N=41)Supplementary Table 2
No Name Symptom ClustersSupplementary Table 3
Other Symptom ClustersSupplementary Table 4
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and/or design acquisition - CYY, AJ, and LJ.
analysis - CYY, AJ, and LJ.
interpretation of the data - CYY, AJ, and LJ.
drafting or critical revision of the manuscript for important intellectual content - CYY, AJ, and LJ.
This study received no external funding. Yun Young Choi received a scholarship from the Brian Korea 21 FOUR Project funded by the National Research Foundation of Korea, Yonsei University, College of Nursing. Jotsna Akter received a scholarship from the United Board for Christian Higher Education in Asia.
A1. Brown JK, Cooley ME, Chernecky C, Sarna L. A symptom cluster and sentinel symptom experienced by women with lung cancer. Oncology Nursing Forum. 2011;38(6):E425-35. https://doi.org/10.1188/11
A2. Chan CW, Richardson A, Richardson J. A study to assess the existence of the symptom cluster of breathlessness, fatigue and anxiety in patients with advanced lung cancer. European Journal of Oncology Nursing. 2005;9(4):325-33. https://doi.org/10.1016/j.ejon.2005.02.003
A3. Chan CW, Richardson A, Richardson J. Managing symptoms in patients with advanced lung cancer during radiotherapy: results of a psychoeducational randomized controlled trial. Journal of Pain and Symptom Management. 2011;41(2):347-57. https://doi.org/10.1016/j.jpainsymman
A4. Chan CW, Richardson A, Richardson J. An investigation of a symptom cluster in Chinese patients with lung cancer receiving radiotherapy. Contemporary Nurse. 2013;45(2):164-73. https://doi.org/10.5172/conu.2013.45.2.164
A5. Chen K, Yang D, Li F, Gao L, Tian Y, Xu B, et al. Changes in the symptom clusters of elderly patients with lung cancer over the course of postoperative rehabilitation and their correlation with frailty and quality of life: a longitudinal study. European Journal Oncology Nursing. 2023;67:102388. https://doi.org/10.1016/j.ejon.2023.102388
A6. Cheville AL, Novotny PJ, Sloan JA, Basford JR, Wampfler JA, Garces YI, et al. Fatigue, dyspnea, and cough comprise a persistent symptom cluster up to five years after diagnosis with lung cancer. Journal of Pain and Symptom Management. 2011;42(2):202-12. https://doi.org/10.1016/j.jpainsymman.2010.10.257
A7. Cheville AL, Novotny PJ, Sloan JA, Basford JR, Wampfler JA, Garces YI, et al. The value of a symptom cluster of fatigue, dyspnea, and cough in predicting clinical outcomes in lung cancer survivors. Journal of Pain and Symptom Management. 2011;42(2):213-21. https://doi.org/10.1016/j.jpainsymman.2010.11.005
A8. Choi S, Ryu E. Effects of symptom clusters and depression on the quality of life in patients with advanced lung cancer. European Journal of Cancer Care. 2018;27(1):e12508. https://doi.org/10.1111/ecc.12508
A9. Fodeh SJ, Lazenby M, Bai M, Ercolano E, Murphy T, McCorkle R. Functional impairments as symptoms in the symptom cluster analysis of patients newly diagnosed with advanced cancer. Journal of Pain and Symptom Management. 2013;46 (4):500-10. https://doi.org/10.1016/j.jpainsymman.2012.09.011
A10. Fox SW, Lyon DE. Symptom clusters and quality of life in survivors of lung cancer. Oncology Nursing Forum. 2006;33 (5):931-6. https://doi.org/10.1188/06.ONF.931-
A11. Franceschini J, Jardim JR, Fernandes AL, Jamnik S, Santoro IL. Relationship between the magnitude of symptoms and the quality of life: a cluster analysis of lung cancer patients in Brazil. Jornal Brasileiro de Pneumologia. 2013;39(1):23-31. https://doi.org/10.1590/s1806-
A12. Gift AG, Stommel M, Jablonski A, Given W. A cluster of symptoms over time in patients with lung cancer. Nursing Research. 2003;52(6):393-400. https://doi.org/10.1097/00006199-
A13. Gift AG, Jablonski A, Stommel M, Given CW. Symptom clusters in elderly patients with lung cancer. Oncology Nursing Forum. 2004;31(2):203-12. https://doi.org/10.1188/04.ONF.203-
A14. Hamada T, Komatsu H, Rosenzweig MQ, Chohnabayashi N, Nishimura N, Oizumi S, et al. Impact of symptom clusters on quality of life outcomes in patients from Japan with advanced nonsmall cell lung cancers. Asia Pacific Journal of Oncology Nursing. 2016;3(4):370-81. https://doi.org/10.4103/2347-
A15. Henoch I, Ploner A, Tishelman C. Increasing stringency in symptom cluster research: a methodological exploration of symptom clusters in patients with inoperable lung cancer. Oncology Nursing Forum. 2009;36(6):E282-92. https://doi.org/10.1188/09.ONF.E283-
A16. Henoch I. The influence of symptom clusters and the most distressing concerns regarding quality of life among patients with inoperable lung cancer. European Journal of Oncology Nursing. 2014;18(3):236-41. https://doi.org/10.1016/j.ejon.2013.12.001
A17. Ju X, Bai J, She Y, Zheng R, Xu X, Wang W, et al. Symptom cluster trajectories and sentinel symptoms during the first cycle of chemotherapy in patients with lung cancer. European Journal of Oncology Nursing. 2023;63:102282. https://doi.org/10.1016/j.ejon.2023.102282
A18. Khamboon T, Pongthavornkamol K, Olson K, Wattanakitkrileart D, Viwatwongkasem C, Lausoontornsiri W. Symptom experiences and symptom cluster across dimensions in Thais with advanced lung cancer. Pacific Rim International Journal of Nursing Research. 2015;19(4):330. https://he02.tci-
A19. Khamboon T, Pakanta I. Intervention for symptom cluster management of fatigue, loss of appetite, and anxiety among patients with lung cancer undergoing chemotherapy. Asia Pacific Journal of Oncology Nursing. 2021;8(3):267-75. https://doi.org/10.4103/2347-
A20. Li JJ, Li JR, Wu JM, Song YX, Hu SH, Hong JF, et al. Change in symptom clusters perioperatively in patients with lung cancer. European Journal of Oncology Nursing. 2021;55:102046. https://doi.org/10.1016/j.ejon.2021.102046
A21. Li N, Wu J, Zhou J, Wu C, Dong L, Fan W, et al. Symptom clusters change over time in patients with lung cancer during perichemotherapy. Cancer Nursing. 2021;44(4):272-80. https://doi.org/10.1097/NCC.0000000000000787
A22. Lin S, Chen Y, Yang L, Zhou J. Pain, fatigue, disturbed sleep and distress comprised a symptom cluster that related to quality of life and functional status of lung cancer surgery patients. Journal of Clinical Nursing. 2013;22(9-10):1281-90. https://doi.org/10.1111/jocn.12228
A23. Liu J, Liu X, Dong M, Zhao H, Li M, Zhang H, et al. Symptom trajectories during chemotherapy in patients with non-small cell lung cancer (NSCLC) and the function of prolonging low dose dexamethasone in promoting enhanced recovery after chemotherapy. Thoracic Cancer. 2021;12(6):783-95. https://doi.org/10.1111/1759-
A24. Ma J, Xu H, Liu S, Wang A. An investigation of symptom clusters and sentinel symptoms during the first 2 cycles of postoperative chemotherapy in patients with lung cancer. Cancer Nursing. 2022;45(6):488-96. https://doi.org/10.1097/ncc.0000000000001058
A25. Maguire R. An interpretative phenomenological analysis of the lived experience of multiple concurrent symptoms in patients with lung cancer: a contribution to the study of symptom clusters. European Journal of Oncology Nursing. 2014; 18(3):310-5. https://doi.org/10.1016/j.ejon.2014.02.004
A26. Molassiotis A, Lowe M, Blackhall F, Lorigan P. A qualitative exploration of a respiratory distress symptom cluster in lung cancer: cough, breathlessness and fatigue. Lung Cancer. 2011; 71(1):94-102. https://doi.org/10.1016/j.lungcan.2010.04.002
A27. Molassiotis A, Vu DV, Ching SSY. The effectiveness of qigong in managing a cluster of symptoms (breathlessnessfatigue-anxiety) in patients with lung cancer: a randomized controlled trial. Integrative Cancer Therapies. 2021;20:15347 354211008253. https://doi.org/10.1177/15347354211008253
A28. Oh IJ, Kim KS, Kim YC, Park JY, Yoo KY, Do SH, et al. Altered hypothalamus-pituitary-adrenal axis function: a potential underlying biological pathway for multiple concurrent symptoms in patients with advanced lung cancer. Psychosomatic Medicine. 2019;81(1):41-50. https://doi.org/10.1097/PSY.0000000000000648
A29. Pudtong N, Aungsuroch Y, Jitpanya C. Symptom clusters in Thai patients with advanced lung cancer. Journal of Health Research. 2014;28(3):183-9. https://he01.tci-
A30. Reyes-Gibby CC, Swartz MD, Yu X, Wu X, Yennurajalingam S, Anderson KO, et al. Symptom clusters of pain, depressed mood, and fatigue in lung cancer: assessing the role of cytokine genes. Supportive Care in Cancer. 2013;21(11):3117-25. https://doi.org/10.1007/s00520-
A31. Russell J, Wong ML, Mackin L, Paul SM, Cooper BA, Hammer M, et al. Stability of symptom clusters in patients with lung cancer receiving chemotherapy. Journal of Pain and Symptom Management. 2019;57(5):909-22. https://doi.org/10.1016/j.jpainsymman.2019.02.002
A32. Sarna L, Brecht ML. Dimensions of symptom distress in women with advanced lung cancer: a factor analysis. Heart Lung. 1997;26(1):23-30. https://doi.org/10.1016/s0147-
A33. Takemura N, Cheung DST, Fong DYT, Ho MH, Lin CC. Relationship between cortisol rhythm and psychoneurological symptom cluster in patients with advanced lung cancer. Cancer Nursing. 2024;47(3):239-45. https://doi.org/10.1097/NCC.0000000000001268
A34.Wang SY, Tsai CM, Chen BC, Lin CH, Lin CC. Symptom clusters and relationships to symptom interference with daily life in Taiwanese lung cancer patients. Journal of Pain and Symptom Management. 2008;35(3):258-66. https://doi.org/10.1016/j.jpainsymman.2007.03.017
A35.Wang D, Fu J. Symptom clusters and quality of life in China patients with lung cancer undergoing chemotherapy. African Health Sciences. 2014;14(1):49-55. https://doi.org/10.4314/ahs.v14i1.8
A36.Wang SY, Tsai CM, Lin CC. Relationship of cytokines to symptom distress and symptom clusters among non-small-cell lung cancer patients receiving gefitinib treatment: a pilot study. Journal of Experimental and Clinical Medicine (Taiwan). 2014;6(2):50-6. https://doi.org/10.1016/j.jecm.2014.02.009
A37.Wang X, Liu J, Duan H, Wei H, Dong Q, Meng Q. Effects of a symptom cluster management intervention on the symptom cluster of pain-cough-fatigue-shortness of breath-anorexia and quality of life among post-thoracoscopic-surgery patients with lung cancer: a randomized controlled trial. Research Square. 2023. Forthcoming. https://doi.org/10.21203/rs.3.rs-
A38. Wong ML, Cooper BA, Paul SM, Levine JD, Conley YP, Wright F, et al. Differences in symptom clusters identified using ratings of symptom occurrence vs. severity in lung cancer patients receiving chemotherapy. Journal of Pain and Symptom Management. 2017;54(2):194-203. https://doi.org/10.1016/j.jpainsymman.2017.04.005
A39. Yorke J, Lloyd-Williams M, Smith J, Blackhall F, Harle A, Warden J, et al. Management of the respiratory distress symptom cluster in lung cancer: a randomised controlled feasibility trial. Supportive Care in Cancer. 2015;23(11):3373-84. https://doi.org/10.1007/s00520-
A40. Yorke J, Johnson MJ, Punnett G, Smith J, Blackhall F, Lloyd Williams M, et al. Respiratory distress symptom intervention for non-pharmacological management of the lung cancer breathlessness-cough-fatigue symptom cluster: randomised controlled trial. BMJ Supportive Palliative Care. 2023;13(e3): e1181-90. https://doi.org/10.1136/spcare-
A41. Zhang G, Weng H, Li Y, Li P, Gong Y, Chen J, et al. Symptom clusters and their predictors in patients with lung cancer and treated with programmed cell death protein 1 immunotherapy. Asian Pacific Journal of Oncololy Nursing. 2022;9(8):100103. https://doi.org/10.1016/j.apjon.2022.100103

 E-SUBMISSION
E-SUBMISSION