
Purpose
Patient outcomes should improve through patient involvement and improved interactions with healthcare providers during the care process. This study aimed to examine factors affecting the perceived health status of patients with cancer, focused on their treatment experiences, and explored the differences in treatment-related experiences according to the patients’ characteristics.
Methods: This cross-sectional study used the 2015 Korea National Health and Nutrition Examination Survey, which assesses patients’ general characteristics, treatment-related experiences, and perceived health status. Data from 255 cancer survivors aged 19 years or older were used in this study. Descriptive statistics, independent t-tests, and multiple regression were used for the data analyses.
Results: Cancer patients’ perception of a lower health resulted from the following factors: insufficient information provision during the care process (β=-.13, p=.026), less participation in the treatment-related decision-making (β=-.25, p=.005), and more comorbidities (β=-.31, p=.018). A higher education level (β=.68, p<.001) was associated with higher perceived health status. The set of significant factors explained 19% of the total variance of the perceived health status.
Conclusion: Sufficient information provision during the care process and patients’ participation in treatment-related decision-making affected the perceived health status of cancer patients. Hence, providing cancer patients with information and involving them in decision-making may improve illness self-management capabilities and health status.
Patient outcomes should improve through patient involvement and improved interactions with healthcare providers during the care process. This study aimed to examine factors affecting the perceived health status of patients with cancer, focused on their treatment experiences, and explored the differences in treatment-related experiences according to the patients' characteristics.
This cross-sectional study used the 2015 Korea National Health and Nutrition Examination Survey, which assesses patients' general characteristics, treatment-related experiences, and perceived health status. Data from 255 cancer survivors aged 19 years or older were used in this study. Descriptive statistics, independent t-tests, and multiple regression were used for the data analyses.
Cancer patients' perception of a lower health resulted from the following factors: insufficient information provision during the care process (β=−.13, p=.026), less participation in the treatment-related decision-making (β=−.25, p=.005), and more comorbidities (β=−.31, p=.018). A higher education level (β=.68, p<.001) was associated with higher perceived health status. The set of significant factors explained 19% of the total variance of the perceived health status.
Sufficient information provision during the care process and patients' participation in treatment-related decision-making affected the perceived health status of cancer patients. Hence, providing cancer patients with information and involving them in decision-making may improve illness self-management capabilities and health status.
Currently, healthcare is undergoing a paradigm shift toward a higher level of patient participation, with a focus on patient-centeredness [1]. Patient-centered care means respecting and responding to individual patient's preferences, needs, and values while ensuring that all clinical decisions made are in accordance with the patient's values and preferences [2]. Patient participation, which generally means “the rights and benefits of the patient having a central position in the care process” is a concept that inevitably accompanies patient-centered care [2]. Therefore, patient participation is essential to patient-centered values. Patient participation has two views: patient involvement should be considered during the healthcare decision-making process [3, 4] and patient involvement refers to acknowledging a patient's feelings about his or her disease treatments and compliance with the healthcare provider's instructions [5].
Patient involvement and improved interactions with healthcare providers during the care process are expected to improve patient outcomes [2]. As equal partners in treatment-related decision-making, patients are encouraged to actively participate in their treatment process and follow treatment plans; thus, better healthcare services are expected to be provided [6]. Many initiatives have been introduced to improve patient participation in care, but patient participation remains challenging for healthcare professionals and the healthcare systems [7]. Therefore, the objective evaluation of patient participation outcomes is necessary.
Previous studies of chronically ill patients' participation outcomes reported that patients' participation in care resulted in better disease control, physical functioning, secondary prevention activities, and perceived health status [8, 9, 10]. A recent study reported that most cancer patients preferred to participate in treatment decision-making and also experienced a high level of shared decision-making. However, cancer patients' actual decision-making participation was inconsistent with their preferences [11]. Participation in treatment decision making among breast cancer patients was associated with improved physical, emotional, and social functions [12] and low depression [13]. Furthermore, the consistency between the preference level of participation in decision-making and the actual participation in patients with breast cancer predicted a higher quality of life [12, 14]. In addition, breast cancer patients who had a more active role in shared decision- making showed higher patient satisfaction and quality of life [15]. Even in patients with ovarian cancer, participation in treatment decision-making was associated with improved emotional functioning and quality of life [16]. Meanwhile, a longitudinal study showed that patients' participation in decision-making had no significant effect on uncertainty and quality of life [17]. Previous results showed controversial positive [12, 13, 14, 15] and negative [11, 17] outcomes of patients' participation in the care process. Moreover, most studies on patients' participation in the care process and outcomes were conducted in the United States [12, 14, 15, 16], Germany [11, 13], and Japan [17]. In addition, most participants from previous studies were patients with breast cancer [12, 13, 14, 15], and some studies focused on patients with ovarian,[16] head, and neck cancer [17]. Therefore, the outcomes of Korean patients with various cancer types who need sufficient information and involvement in the complicated care process should be evaluated. Moreover, it must be explored whether treatment experiences would be different according to the patient's characteristics.
The Korea National Health and Nutrition Examination Survey (KNHANES) uses a probability sampling method and produces reliable national- and provincial-level statistics on the health status and behavior of Koreans [18]. The 2015 KNHANES collected data on patients' treatment experiences including consultation with healthcare providers, understandable explanations, opportunity to ask questions, patients' participation in treatment decision making, and perceived health status. KNHANES did not collect data on these variables during other years.
The purpose of this study was to examine factors affecting cancer patients' perceived health status, treatment experiences, and differences in treatment-related experiences according to patients' characteristics using the 2015 KNHANES data.
This study employed cross-sectional study design and secondary data analyses.
The data were collected from the subjects registered in the 2015 KNHANES. Cancer types included in this study were stomach cancer, liver cancer, colorectal cancer, breast cancer, cervical cancer, lung cancer, thyroid cancer, and other cancers (ovarian cancer, brain tumor, pituitary tumor, lymphoma, bone cancer, multiple myeloma, gallbladder cancer, biliary tract cancer, bladder cancer, leukemia, genital cancer, small intestine cancer, esophageal cancer, kidney cancer, uterine cancer, prostate cancer, pancreatic cancer, salivary gland cancer, skin cancer, laryngeal cancer, and thymus cancer). Study participants aged 19 years and older were selected based on their cancer diagnosis, and patients diagnosed with depression were excluded.
A total of 7,380 patients were enrolled in the 2015 KNHANES. Cancer patients aged 19 years and older were initially selected (n=271). Those who were diagnosed with depression were excluded (n=16) due the impact depression can have on the treatment-related decision-making process. Ultimately, 255 patients were included in the analysis.
The Korea Centers for Disease Control and Prevention (KCDC) conducts the KNHANES annually. This survey is a national representative sample obtained by stratified random sampling and cluster sampling. The units for stratified random sampling were gender and age. Cluster random sampling was a multistage procedure that considered the geographical area of residence based on household registries. In this study, the data were obtained from three surveys of KNHANES: health interview, health examination, and nutrition survey. The health interview and health examination were performed in a vehicle-based examination center, whereas the nutrition survey was conducted during scheduled household visits. All participants provided written informed consent before participation. A subset of the KNHANES data was used, and participants were not directly contacted. The KCDC complies with the Personal Information Protection Act and Statistics Act and only provides data that have been de-identified to maintain participants' anonymity from the survey data. The data can be downloaded from the KNHANES website (https://knhanes.cdc.go.kr/knhanes/main.do) and used for academic research purposes.
General characteristics included the following: age, gender, residential area (city or rural), monthly household income, job, marital status, education level, health insurance type, basic living recipient, cancer type, and number of years since the cancer diagnosis. The number of comorbidities, treatment experience within the last year, and main type of outpatient institution used were determined from the 2015 KNHANES raw data.
The main independent variables were addressed in four treatment-related experience questions focusing on the patient's experience with sufficient time for information provision, clear explanation, opportunity to ask questions, and participation in decision-making. The four questions were answered using a 4-point Likert scale consisting of always (1), usually (2), sometimes (3), and not at all (4). A higher score indicates less opportunity to ask questions and less experience in decision-making participation. Specific questions were “Did your healthcare provider take sufficient time to provide you information?”, “Have you been given an easy-to-understand explanation?”, “Have you been given the opportunity to ask questions or concerns about your treatment?”, and “When making a decision on your treatment, has your opinion been reflected?”
The dependent variable was a question about perceived health status. The specific question was “How do you usually rate your health?”, and the response options were very good (5), good (4), moderate (3), poor (2), and very poor (1) (5-point Likert scale). A higher score indicates a better perceived health status.
The KNHANES was approved by the Institutional Review Board (IRB) of the KCDC, conforming to the principles of the Declaration of Helsinki, which was revised in 2000. The KNHANES data used in this study are public, but the identities of all respondents remain anonymous. The study protocol was exempt from the research ethics review process of the K University Research Ethics Review Committee. Ethical approval for this study was waived by the IRB of K University in accordance with the waiver reason “research using information open to the general public”( no. KNU-2020-0120).
All estimates were weighted analyses obtained through statistically weighted values provided by the KCDC, which was adjusted for the sample design and response rate (Korea Centers for Disease Control and Prevention, 2012). All statistical data were analyzed using the SURVEY PROCEDURE command in SAS 9.4 (SAS Institute Inc., Cary, NC). Descriptive statistics on weighted values were calculated using the PROC SURVEYMEANS and PROC SURVEYFREQ commands, whereas those on sample values were calculated with PROC FREQ and PROC MEANS. To compare the differences in treatment-related experiences according to patients' characteristics, an independent t-test was performed; to examine the factors affecting perceived health status, a multiple regression analysis was conducted. At the exploratory stage, confounding factors were identified by the independent t-test. These confounding factors were significantly associated with sufficient consulting time, easy-to-understand explanations, opportunity to ask questions, and involvement in treatment-related decision -making. According to existing literature, the included covariates were age, gender, monthly household income, marital status, residence area, job, education level, health insurance, ever basic living recipient, years since cancer diagnosis, number of comorbidities, and type of medical institution used [19, 20, 21]. Then, significant covariates (p≤.05) in the univariate analysis were entered into a stepwise multiple regression model. The best subset of independent variables was identified by the stepwise selection method for the outcome variable (i.e., perceived health status). Missing data were excluded in analyzing multiple regression. The results of the multiple regression analyses are expressed by regression coefficients (β) and their Standard Errors (SEs), partial R2 (amount of variance in each predictor associated with the outcome), and total R2 (total variance of all predictors associated with outcome). All statistical tests were two-tailed, and p-values less than .05 were considered significant.
More than half of the patients were below 65 years old (56.9%), women (56.4%), had a monthly household income of over $2,000 (57.4%), had a high school or higher educational level (52.5%), and were diagnosed with cancer for over 5 years (59.3%). Three-quarters of patients lived with their spouse (74.3%) and resided in the city (77.2%). Most of the patients were enrolled in health insurance (95.7%) and never received basic living benefits (93.5%). In addition to cancer, three or more other comorbidities were found in 36.9% of patients. Patients with gastric cancer accounted for the largest proportion (22%), followed by thyroid cancer (18.2%), and breast cancer (13.1%). Moreover, more than half of the patients used general hospitals within the last year (59.2%) (Table 1).
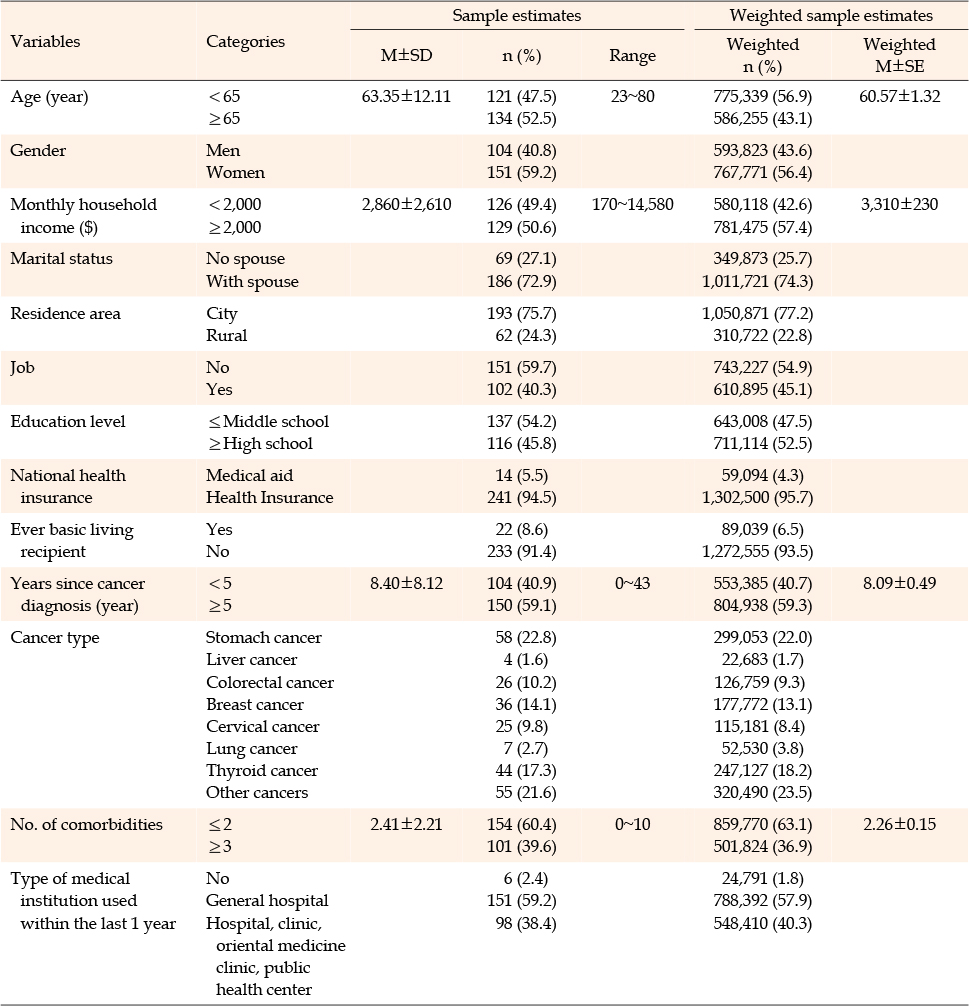
Table 1
General Characteristics of the Sample (N=255)
Patients who were age (p<.001), had lower income (p=.007), had a lower educational level (p<.001), and were medical aid recipients (p<.001) reported that they were provided with sufficient time for information provision. Patients with a spouse (p=.017), low educational level (p=.004), medical aid recipients (p=.001), and additional comorbidities (p=.011) were reportedly provided with easy-to-understand explanations. Those with lower educational levels (p<.001) and medical aid recipients (p<.001) reported that they received sufficient opportunities to ask questions. Those with older age (p=.004), a lower educational level (p<.001), medical aid (p=.005), and more comorbidities (p=.009) reported that they were more involved in treatment-related decision-making (Table 2).
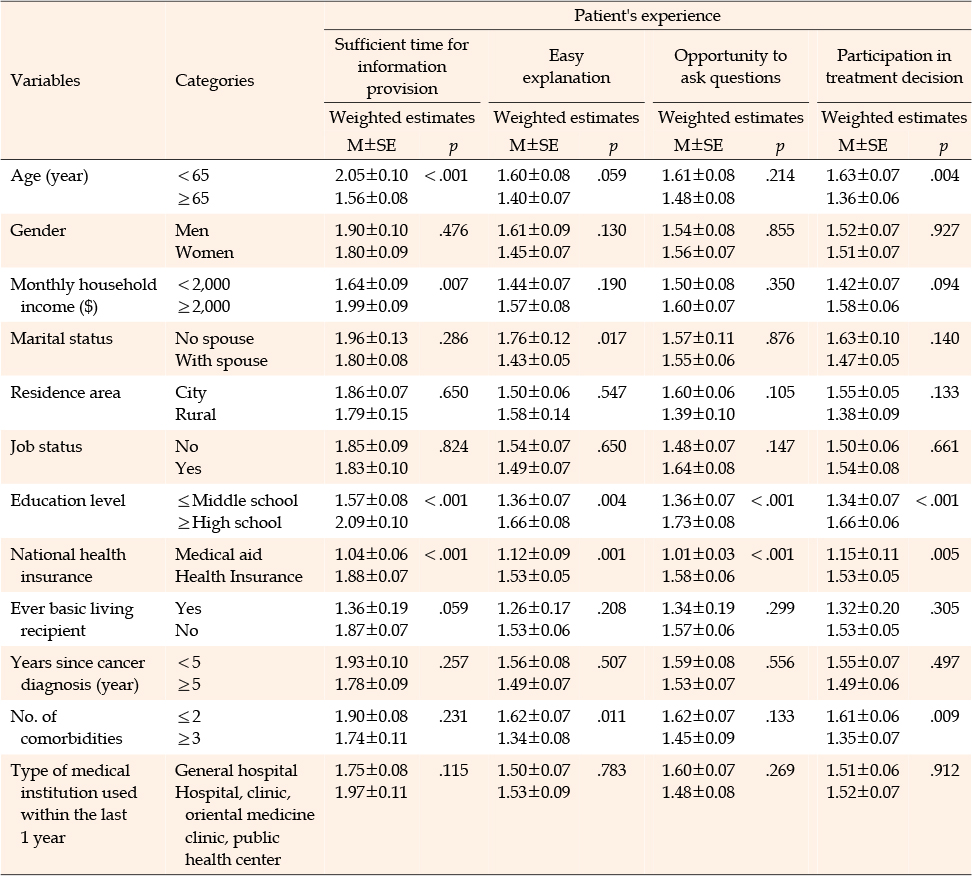
Table 2
Differences in Treatment-related Experiences according to Patient's Characteristics (N=255)
Multicollinearity was tested before the multiple regression analysis. Variance inflation factors ranged from 1.14 to 2.20, and tolerance ranged from .45 to .88; thus, the predictor variables had no multicollinearity. The Durbin-Watson statistic was 1.91 (p=.243), which indicated no autocorrelation among predictor variables.
Variables that were significant in the univariate analyses (Table 2), such as age, education, medical aid recipient, marital status, and comorbidities were associated with a lower perceived health status among cancer patients. This low perception was accompanied by insufficient explanations during the care process (β=−.13, p=.026), less involvement in treatment-related decision-making (β=−.25, p=.005), and additional comorbidities (β=−.31, p=.018). Meanwhile, a higher education level (β=.68, p<.001) was associated with a higher perceived health status. The set of significant factors explained 19% of the total variance of the perceived health status (Table 3).
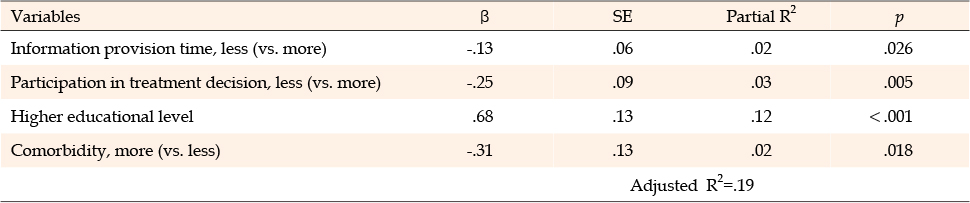
Table 3
Factors Affecting Patients' Perceived Health Status (N=255)
This study examined the influence of treatment experiences on patient's perceived health status. Results revealed that patient involvement during the care process affected the perceived health status among cancer patients.
Sufficient explanations during the care process and involvement treatment-related decision-making may result in better perceptions of health status among cancer patients. This result was well-supported by previous studies involving cancer survivors [12, 22, 23, 24, 25]. Satisfaction with information received or fulfillment of information needs was associated with overall health [22], better illness perceptions [23], and better quality of life [12, 24]. When cancer survivors are provided with satisfactory treatment information and sufficiently involved in healthcare decision-making, they develop coping abilities and control over the disease and the adverse effects of cancer treatments. In addition, involvement healthcare decision-making increases patient satisfaction, reduce anxiety about treatment, and promote emotional stability [25]. Therefore, patient satisfaction with information provision demonstrates a significant relationship with the patient's perceived health.
This study examined how the treatment experiences vary based on the patients' sociodemographic characteristics. Older patients reported that they were provided with sufficient time for information provision, and they were more involved in treatment-related decision-making. Patients with lower educational levels, medical aid, and lower income reported that they were provided with sufficient time for information provision, easy-to-understand explanations, sufficient opportunities to ask questions, and opportunities for treatment-related decision-making. Cancer patients reported that they preferred and had a collaborative role in treatment-related decision-making. However, less-educated older patients with lower incomes were more likely to prefer a passive role [12, 20, 26] in treatment decision-making, such as following healthcare professionals' recommendations or suggestions. Lower education levels, old age, and low income were associated with poor knowledge about the care process [27]. Lower education levels and lower income were associated with the feeling of well-informed about medication and screening decisions [28]. In general, people with more expertise tend to adjust better and perform better self-evaluations. Patients with lower education levels and lower income are less likely to perceive their knowledge deficits; consequently, they may not have the need to seek information [28].
Cancer patients with more comorbidities reported that they were provided with easy-to-understand explanations and more involved in treatment-related decision-making. Older patients with comorbidities who suffer serious side effects after the first chemotherapy are more involved in the decision-making process by inquiring about their side effects prior to undergoing additional treatments [29]. People with many comorbidities are more likely to experience adverse reactions during and after surgery and chemotherapy. Therefore, the patient may have a different decision regarding surgery and selection of anticancer drugs, which complicates decision-making. These patients' values preferences might be reflected in the treatment-related decision-making process through sufficient explanation. Patients who had a lower educational level and multiple comorbidities were less likely to be provided with sufficient time for information provision by healthcare providers, easy-to-understand explanations, an opportunity to ask questions, and involvement in treatment-related decision-making. Finally, the passive participation in treatment decision-making among patients with less education and with more comorbidities could lead to a negative perception of their health status.
In this study, patients' involvement in treatment decisions, educational level, comorbidities, and healthcare providers' time for information provision explained 19% of the total variance of perceived health status, and the explanatory power was relatively low. Although various factors determine the health status of cancer patients including complications, treatment sequelae, symptom management, healthy lifestyle, exercise and nutrition, information provision, and education, this study focused on the treatment experience during the care process as a potential predictor of perceived health status. This is also a possible reason for low explanatory power.
These results need to be interpreted based on the following study limitations. First, this study is cross-sectional in design. Due to the limitation of cross-sectional studies, there are possibly additional confounding variables that could not controlled in this study while examining the association between the treatment experience and health status of cancer patients. Therefore, result interpretations are limited to a causal relationship or generalized findings. Future studies on treatment experiences and outcomes require a longitudinal design. Second, patients' experiences related to treatment within the last year were surveyed. These experiences reflect the patients' knowledge during information provision and decision-making during the care process. In addition, a patient may forgotten part of the treatment process and responded according to his or her overall perception, which indicates recall bias. However, analyzing the data collected closer to the time of treatment- related decision-making does not necessarily support the researcher's hypothesis [30]. This is because patients' perception becomes stronger over time, and they tend to justify and reinforce their choices and decisions. Eventually, previous care experiences may be related to patients' perception [30].
Nurses and other oncology clinicians can clarify the patient's preferred role in the treatment-related decision-making process. Nurses can ensure that patients are provided with treatment-related information, encourage patients to express their preferred role in the decision-making process to the physician, and develop treatment-related decision-making autonomy. Nurses can develop a culture of mutual respect and value for needs and support treatment-related decision-making throughout the continuity of care.
It is possible to improve point-of-care, improve patient outcomes, and ultimately contribute to the improvement of health nationally by utilizing big data on treatment experiences (i.e., KNHANES).
In conclusion, patients' perception of the adequacy of explanations provided during the care process and involvement in the treatment-related decision-making helped achieve an improved health status perception among cancer patients. Age, educational level, income, and comorbidity were associated with patients' treatment experiences. Providing sufficient time for information provision and involving patients in decision-making during the care process, particularly among patients with low educational levels and multiple comorbidities, might be necessary to improve their perceived health status. Further research is needed to determine the degree of concordance between the preferred involvement level in treatment-related decision- making and the patient's actual involvement in the decision-making process, which affects their health and quality of life. In addition, intervention studies on the effects of tailored decision-making that aids cancer survivors in achieving health-related quality of life and patient outcomes are also needed.
CONFLICTS OF INTEREST:The author declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition, Data extraction, Analysis and interpretation of the data, Drafting and critical revision of the manuscript - LMK
This research was supported by Kyungpook National University Research Fund, 2020.
 E-SUBMISSION
E-SUBMISSION