
Purpose
This study aimed to examine the effects of health-related behaviors on metabolically healthy non-obese or obese groups and to analyze gender differences.
Methods
This study was a secondary descriptive study. A total of 14,277 adults from the Korea National Health and Nutrition Examination Survey 2013~2015 were classified as: metabolically healthy non-obese; metabolically unhealthy non-obese; metabolically healthy obese; or metabolically unhealthy obese. Five health-related behaviors (amount of alcohol consumption, smoking status, physical activity, daily energy intake, and sleep duration) were included as independent variables.
Results
The health-related behaviors associated with metabolic status in non-obese participants were drinking and smoking, whereas those of obese individuals were associated with physical activity. Subgroup analysis showed that more metabolically healthy non-obese men were light drinkers and former smokers than metabolically unhealthy non-obese men.
Metabolically healthy non-obese women were more likely to engage in physical activity than metabolically unhealthy non-obese women. Among the obese men, light drinking and physical activity were associated with metabolic status.
Conclusion
Evidence-based interventions promoting health-related behaviors are needed to support metabolic health, considering the metabolic status and obesity phenotypes of the participants and their gender.
This study aimed to examine the effects of health-related behaviors on metabolically healthy non-obese or obese groups and to analyze gender differences.
This study was a secondary descriptive study. A total of 14,277 adults from the Korea National Health and Nutrition Examination Survey 2013~2015 were classified as: metabolically healthy non-obese; metabolically unhealthy non-obese; metabolically healthy obese; or metabolically unhealthy obese. Five health-related behaviors (amount of alcohol consumption, smoking status, physical activity, daily energy intake, and sleep duration) were included as independent variables.
The health-related behaviors associated with metabolic status in non-obese participants were drinking and smoking, whereas those of obese individuals were associated with physical activity. Subgroup analysis showed that more metabolically healthy non-obese men were light drinkers and former smokers than metabolically unhealthy non-obese men. Metabolically healthy non-obese women were more likely to engage in physical activity than metabolically unhealthy non-obese women. Among the obese men, light drinking and physical activity were associated with metabolic status.
Evidence-based interventions promoting health-related behaviors are needed to support metabolic health, considering the metabolic status and obesity phenotypes of the participants and their gender.
Obesity is a major public health concern. It is one of the leading causes of cardiovascular disease, diabetes, and some cancers, and its prevalence among adults is rapidly growing globally [1]. However, recent studies found that neither cardiovascular mortality [2] nor all-cause mortality [3] increased in a Metabolically Healthy Obese (MHO) group when compared with a Metabolically Healthy Non-obese (MHNO) group, while a Metabolically Unhealthy Non-obese (MUNO) or Metabolically Unhealthy Obese (MUO) group had a higher risk.
Health-related behaviors, such as alcohol consumption, smoking [4], physical activity, caloric intake [5], and sleeping duration [6] are the most important factors in the prevention and management of metabolic syndrome because they affect visceral fat. Thus, health-related behaviors by the four metabolic status-obesity phenotypes might significantly influence and differentiate the prognosis of each group. However, few studies have investigated the differences in health-related behaviors among all metabolic statuses and obesity phenotypes, and results have been inconsistent. For example, physical activity [7], healthy diet [8], less alcohol consumption, and noncurrent smoking [9] have been found to be related to MHO rather than MUO. However, some studies have found that health-related behaviors are not associated with metabolically healthy phenotypes [10], and unhealthy behaviors such as smoking have also been observed in metabolically healthy groups [11]. In addition, almost no studies have made gender distinctions, even though the patterns of health-related behaviors between men and women were different. For example, the smoking rate in men was reported more than five times higher than that in women [12]. This gender difference in health-related behaviors might affect metabolic status and obesity phenotypes. As shown in the application of different cut-off points for diagnosing metabolic syndrome in men and women [13], the characteristics of metabolic status are different. Therefore, it is necessary to analyze the health-related behaviors affecting the MHNO or MHO groups, which have a better prognosis than the MUNO or MUO groups, and further examine gender-specific characteristics. The aims of this study were 1) to examine whether health-related behaviors were associated with the MHNO or MHO groups, compared with the MUNO or MUO groups, and 2) to identify any gender differences in the relationship between health-related behaviors affecting metabolic status and obesity phenotypes.
This study was a secondary data analysis using data from the 6th Korea National Health and Nutrition Examination Survey (KNHANES VI).
We analyzed data from KNHANES VI, which were collected between 2013 and 2015. KNHANES VI is a population-based national survey on health and nutritional status conducted by the Korea Disease Control and Prevention Agency (KDCA) every three years. KNHANES VI used a cross-sectional stratified multistage cluster sample survey method. After the first extraction using the census, the target population was selected by extracting households. The investigator visited participants in person on a mobile screening vehicle, and a computer-assisted personal interviewing method was used [14].
In KNHANES VI, 22,948 participants were recruited from 9,491 households. In our study, we included only 15,397 adults aged ≥19 years for whom there were no missing values for metabolic measurements and Body Mass Index (BMI). From this sample, we excluded 1,120 participants: 44 pregnant women who had specific guidelines for obesity depending on the stage of pregnancy and 1,076 participants with cancer, myocardial infarction, stroke, liver cirrhosis, or renal failure diagnoses because these individuals might be undergoing therapeutic lifestyle modification [15]. Finally, 14,277 adults from the KNHANES VI were included in this study (Figure 1).
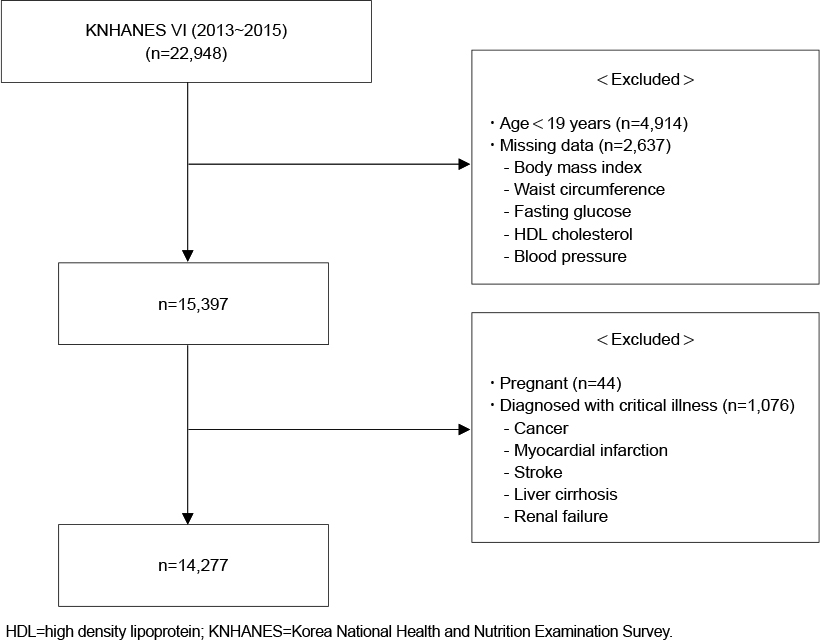
Figure 1
Flow sheet of exclusion criteria.
The study protocols were approved by the institutional review board of Yonsei University Health System (IRB No. Y-2018-0079) before the study began. As KNHANES VI provides anonymized data based on the Personal Information Protection Law, it is not feasible to identify a specific person, and therefore informed consent was not required.
Participants were classified into four groups according to obesity and metabolic status: MHNO, MUNO, MHO, and MUO. Obesity was defined according to BMI based on the Korean Society for the Study of Obesity (KSSO) guidelines of ≥25 kg/m2, indicating obesity [16]. It is necessary to use strict BMI cut-off points for obesity in Asians because Asians have a higher risk of cardiovascular disease than Westerners [17]. Metabolic status was classified using the modified National Cholesterol Education Program Third Adult Treatment Panel (NCEP-ATP-III)[13]. For waist circumference, we followed the criteria from the KSSO [16]. Following the modified NCEP-ATP III, we defined metabolic abnormalities as a high waist circumference (>90 cm for men and >85 cm for women), impaired fasting glucose (≥100 mg/dL), hypertriglyceridemia (≥150 mg/dL), low High Density Lipoprotein (HDL) cholesterol (<40 mg/dL for men and <50 mg/dL for women), and elevated blood pressure (systolic ≥130 mmHg or diastolic ≥85 mmHg). A metabolically healthy status was defined as having fewer than three abnormal factors, while a metabolically unhealthy status was defined as having three or more abnormal factors.
Based on these definitions, participants were divided into (i) MHNO: BMI <25 kg/m2 and <3 metabolic abnormalities; (ii) MUNO: BMI <25 kg/m2 and ≥3 metabolic abnormalities; (iii) MHO: BMI ≥25 kg/m2 and <3 metabolic abnormalities; and (iv) MUO: BMI ≥25 kg/m2 and ≥3 metabolic abnormalities.
We included the amount of alcohol consumption, smoking status, physical activity, daily energy intake, and sleep duration as health-related behavioral variables. The amount of alcohol consumed was divided into two groups, based on the total volume of alcohol consumed in one drinking session: 40 g alcohol or above and less than 40 g alcohol [18]. Smoking status was categorized as current smoker, former smoker, or never smoker. Physical activity was defined as moderate-intensity physical activity performed for at least 150 min per week or high-intensity physical activity performed for at least 75 min per week [19]. Daily energy intake was classified as insufficient energy intake and excess energy intake, based on the recommended levels of energy intake by Ministry of Health and Welfare, Korea [20]: for men, aged 19~29=2,700 Kcal, aged 30~49=2,400 Kcal, aged 50~64=2,200 Kcal, aged 65 or older= 2,000 Kcal; for women, aged 19~29=2,100 Kcal, aged 30~49=1,900 Kcal, aged 50~64=1,800 Kcal, aged 65 or older= 1,600 Kcal. Sleep duration was assessed using the question “How many hours per day do you sleep on average?” We classified answers into two groups: sleeping less than seven hours and seven hours or more per day [6].
Demographic and socioeconomic covariates included gender, age, level of education, level of income, and type of work shift. The level of education was defined as a categorical variable: high school education or less and college education or above. The level of income was divided into three groups based on individual income: high for the first quartile, medium for the second and third quartiles, and low for the fourth quartile. Finally, shift work was categorized into three groups: day work, night work, and shift work.
The health and nutrition survey was a self-reported questionnaire including socioeconomic characteristics, current health conditions, and health-related behaviors such as drinking, smoking, physical activity, energy intake, and sleeping.
Clinical examinations, including medical and physiological measurements, were performed by trained personnel according to standardized guidelines [14]. BMI was calculated as weight in kilograms (GL-6000-20, Gtech International, Gyeonggi-do, Korea) divided by the square of height in meters (Seca 225, Seca, Hamburg, Germany). Waist circumference was measured between the bottom of the lowest rib and top of the iliac crest (Seca 200). Blood pressure was measured by KDCA nurses thrice using a Baumanometer Wall Unit 33 (WA Baum, NY, USA). For the analyses, we used the mean values of the last two measurements. Blood samples were collected after at least eight hours of fasting for fasting glucose, triglyceride, and HDL cholesterol measurements.
Since the KNHANES extracted samples using a complex sample survey design, sample weights, strata, and clusters were applied to all analyses. Data were described as frequencies with percentages or means with Standard Errors (SE) to consider the participants as representative of the population after adjustments for the 2013~2015 weights data. Individual characteristics and health-related behaviors were compared between the MHNO and MUNO, and between MHO and MUO individuals, using the weighted χ2 test or independent t-test.
In dichotomizing participants into obese and non-obese groups, complex sample multiple logistic regression was performed to estimate the Odds Ratios (ORs) for the associations between health-related behaviors and metabolic status. The following socioeconomic factors related to metabolic status were included in the adjusted analysis: gender, age, level of education, level of income, and work shift. Additionally, we analyzed the relationship between metabolic status and health-related behavior by gender to identify potential differences. All analyses were performed using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
1. Participants’ Characteristics according to Metabolic Status-Obesity Phenotype
Table 1 shows participants’ characteristics according to their metabolic and obesity status. Of the 14,277 participants, 60.4% were classified as MHNO (n=8,426; weighted n=21,071,102), 6.9% were MUNO (n=1,150; weighted n=2,391,386), 17.8% were MHO (n=2,460; weighted n=6,195,164), and 14.9% were MUO (n=2,241; weighted n=5,214,178). In both the non-obese and obese groups, participants identified as metabolically healthy were significantly younger and had more than a college-level education. Compared with the MUNO group, the MHNO group had more women, fewer participants with a high level of income, and fewer day workers.
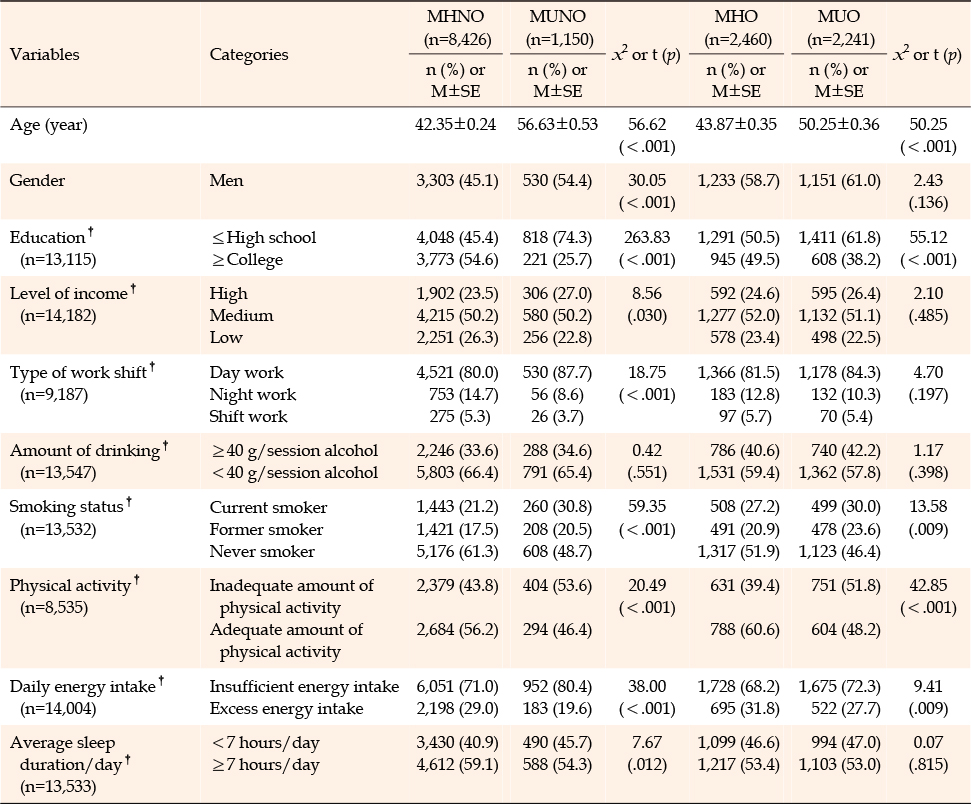
Table 1
Participants' Characteristics according to Metabolic Status-Obesity Phenotype (N=14,277)
In the MHNO and MHO groups, there were fewer current smokers and more participants with adequate amounts of physical activity and excess energy than in the MUNO and MUO groups, respectively. MHNO participants, as compared to MUNO participants, had a greater likelihood to sleep more than 7 hours a day (Table 1).
In both the non-obese and obese groups, the odds ratio of being metabolically healthy were higher in younger individuals. Among the non-obese groups, women were more likely to have MHNO status than men. Socioeconomic factors were not significantly associated with metabolic status in multivariate logistic regression analysis.
Among non-obese adults, the odds ratio of being MHNO increased 1.79 times (95% Confidence Interval [CI] 1.35~2.37) in those who engaged in light drinking, and 1.59 times (95% CI 1.08~2.34) in former smokers. Among obese adults, the odds ratio of being MHO was 1.32 times (95% CI 1.09~1.68) higher when engaging in physical activity (Table 2).
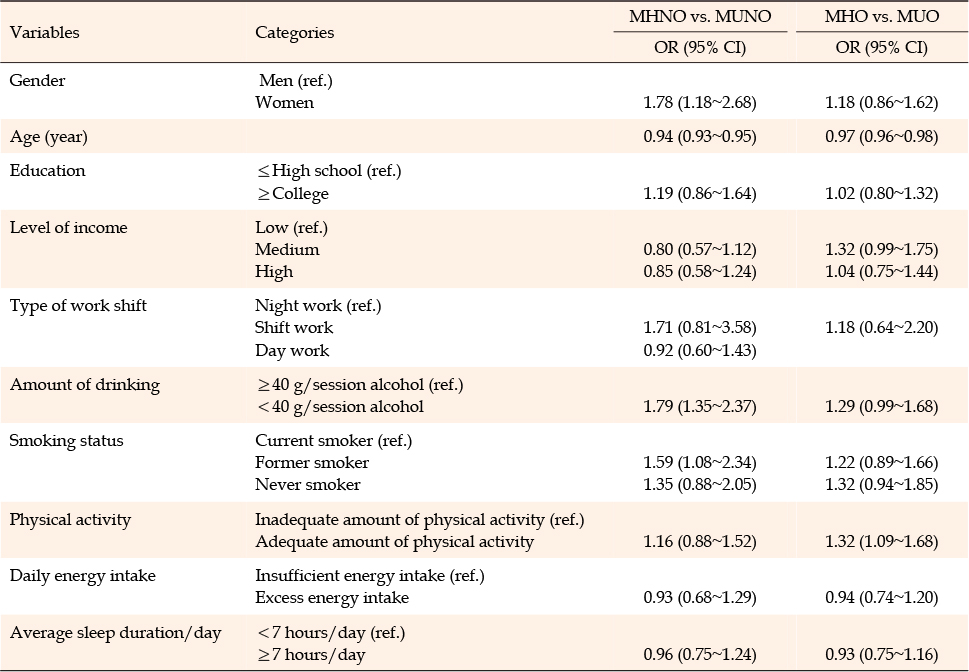
Table 2
Association between Metabolic Status and Health-Related Behaviors
The results among men were similar to the general results: among non-obese men, drinking less alcohol (OR 1.90, 95% CI 1.36~2.66) and being a former smoker (OR 1.47, 95% CI 1.00~2.16) were associated with increased odds of being MHNO; among obese men, participants who drank less alcohol had 1.52 times (95% CI 1.13~2.03) higher odds of being MHO, while those who engaged in adequate amounts of physical activity had 1.61 times higher odds (95% CI 1.22~2.12) of being MHO (Table 3).
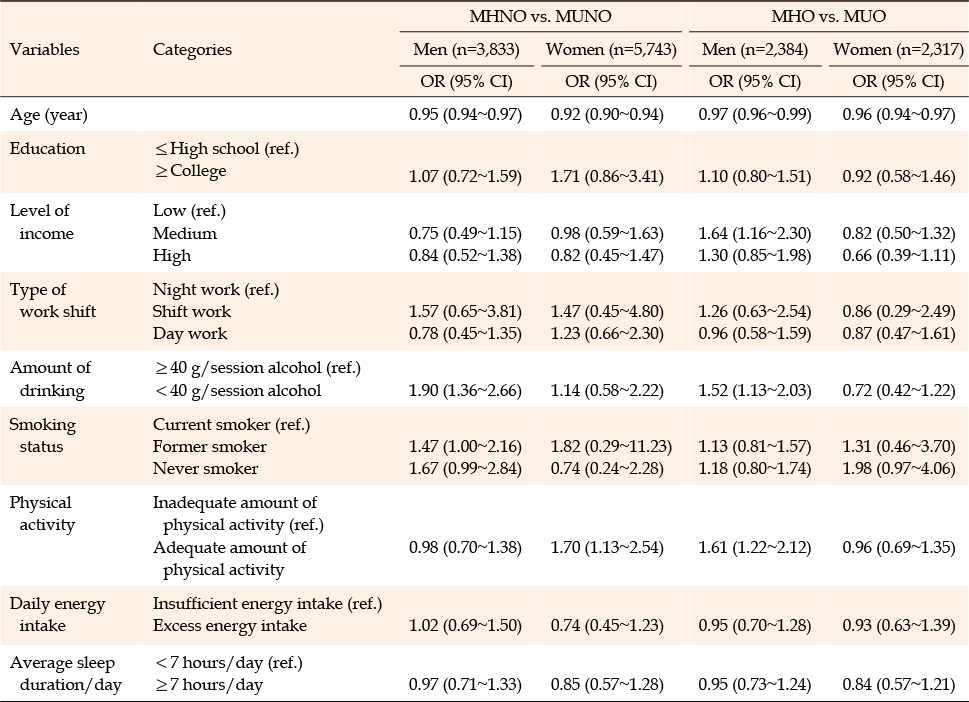
Table 3
Association between Metabolic Status and Health-Related Behaviors by Gender
Among non-obese women, physical activity was positively associated with metabolic health (OR 1.70, 95% CI 1.13~2.54). However, we found no statistically significant association between health-related behaviors and the MHO phenotype among obese women.
This study revealed that different health-related behaviors were associated with MHNO or MHO phenotypes, compared with MUNO or MUO phenotypes in the general population. Specifically, light alcohol consumption and former smoking were associated with metabolic health among the non-obese group, while only adequate physical activity was associated with metabolic health among the obese group. These findings were consistent with those of previous studies that identified health-related behaviors between metabolic status and obesity phenotypes [9, 21]. A study conducted in a Korean tertiary medical center reported that the proportion of current smokers and moderate drinkers was significantly lower in the MHNO and MHO groups than in the MUNO and MUO groups. The ratio of physical activity was higher in the MHO group than in the MUO group [9]. In a Spanish study, heavy drinking, former or current smoking, and a lack of physical activity were factors that increased the odds ratios of being classified as metabolically unhealthy phenotypes [21].
One possible explanation for these results is related to the Visceral Adiposity Index (VAI), a widely used indicator of adipose tissue dysfunction [22]. The level of VAI rises when metabolic health is impaired [22], and it has also been found that MHO participants with high VAI were more likely to convert to MUO after a few years [9]. Since alcohol consumption and smoking are significant factors that increase VAI [23], and physical activity lowers VAI [24], it could be considered that these health-related behaviors were related to metabolically healthy phenotypes, compared with metabolically unhealthy phenotypes.
Daily energy intake and sleep duration had no significant effect on metabolic health in either the obese or non-obese group. Similarly, there was no difference in energy intake between the MHO and MUO groups in an Irish study [25]. This might be because the glucose and insulin responses of the MUO group were lower than those of the MHO group, even though the MHO and MUO groups consumed the same standardized diet [26]. Regarding sleep, a large cross-sectional study found no significant relationship between sleep duration and MHO phenotype [27]. However, since there are extremely few studies on the correlation between energy intake, sleep duration, and metabolic status among non-obese and obese groups, further studies are needed to improve our understanding.
In this study, there were gender differences in health-related behaviors affecting the expression of the MHNO or MHO phenotypes. Among men, a lower amount of alcohol consumption and former smoking were correlated with MHNO as opposed to MUNO, while lighter drinking and physical activity were associated with MHO as opposed to MUO. Among women, those who underwent adequate amounts of physical activity had higher odds of being in the MHNO phenotype than the MUNO group. In contrast, there was no significant association between health-related behaviors and MUO phenotype in obese women. Alcohol consumption and smoking status were related to metabolic health only in men. According to a previous study, co-smokers and drinkers showed higher VAI than non-drinking smokers [23]. Therefore, among men with a high rate of heavy drinking and smoking, alcohol consumption and smoking status had a greater effect on metabolic state. However, weight gain after smoking cessation [28] might have offset the positive effects of smoking cessation in obese men. Physical activity was also a significant determinant of metabolic status in obese men and non-obese women. This might have been related to the fact that moderate to vigorous physical activity decremented a larger amount of visceral adipose tissue in women than in men [29].
Unexpectedly, no health-related behaviors were significantly correlated with the metabolic status of obese women. Similar results were found in a Taiwanese cross-sectional study, in which none of the lifestyles and dietary habits, apart from dairy consumption, was associated with metabolic status in women [30]. This may be related to oxytocin deficiency, which is a typical characteristic among obese women. Oxytocin deficiency causes metabolic impairments, such as increased insulin resistance and increased low density lipoprotein levels [31]. However, we did not consider the hormonal profiles of the women in our study because of the limitations of KNHANES VI variables. Managing metabolic syndrome in obese women might require treatment that considers the hormonal profile instead of simple behavioral treatment.
Although a previous study reported that shift workers had an increased risk of metabolic syndrome [32], shift work did not affect metabolic status in this study. Deng et al.[32] hypothesized that shift work increases the risk of metabolic syndrome due to sleep deprivation; however, Korea has unique working conditions due to fierce competition. The average annual working time in Korea is 2,024 hours per worker, the third highest among the Organization for Economic Co-operation and Development countries [33]. Due to overwork, most Koreans regularly engage in overtime at night, which might explain why shift work is not associated with metabolic status. Further research is needed to identify socioeconomic factors associated with metabolic status and obesity phenotypes in Korea.
There were several limitations to this study that must be considered when interpreting our findings. The design of the KNHANES VI was cross-sectional, and we were unable to prove causal relationships between the variables. Additionally, unhealthy behaviors could have been under-reported because data were based on self-reporting. Finally, potential covariates, such as hormonal profiles, were not available in the KNHANES VI. Despite these limitations, this study used a representative population-based survey of the Korean population. Thus, it is possible to estimate the association between health-related behaviors of Korean adults and their metabolic status and obesity. Our findings indicate that light alcohol consumption, smoking cessation, and adequate physical activity have a positive effect on the expression of metabolically healthy phenotypes. However, the current metabolic guidelines published by the KSSO only introduced dietary intervention, physical activity, and weight loss as lifestyles for the prevention and treatment of metabolic syndrome [16]. The importance of consuming less alcohol and smoking cessation should also be emphasized. In addition, nurses should emphasize the importance of reducing alcohol consumption, smoking cessation, and physical activity when providing metabolic health education for Korean adults.
Health-related behaviors were associated with different types of metabolic status-obesity phenotypes and differed by gender. Evidence-based interventions promoting lifestyle modifications are needed to support metabolic health. In particular, nurse-led interventions tailored by gender and metabolic status-obesity phenotype would be beneficial. For instance, promotion of a low-risk drinking culture or a program for smoking cessation may be beneficial for men. In addition, for those who practice smoking cessation, a weight gain prevention program may be needed.
CONFLICTS OF INTEREST:The authors declared no conflict of interest.
AUTHORSHIP:
Study conception and design acquisition - JH and LKH.
analysis and interpretation of data - JH and LH.
drafting and critical revision of the manuscript - JH, LKH, JY and LH.
All authors approved the final version of manuscript.
This article is based on a part of the first author's master's dissertation from Yonsei University.
 E-SUBMISSION
E-SUBMISSION